Can the Obesity Crisis Be Reversed?
From conclusions:
Ending the obesity epidemic will take both individual and collective action. Neither alone is sufficient. Individuals try to lose weight and keep it off, but the system is working against them. The route to population-wide weight loss will not be through trendy, unsustainable diets. It will be through widespread, appropriate, personalized, and comprehensive approaches.
The first action we all must take, no matter our size, is to educate ourselves about obesity—and you’ve been doing that by reading this book. People need to understand the structural, environmental, and genetic components of obesity. They need to see the ways in which systemic factors contribute to weight gain. The idea that obesity is a choice or a matter of willpower has been thoroughly disproved. The unfortunate fact that many people still believe this actively harms efforts to reduce obesity rates.
The government should first seek to change the public perception of obesity. Obesity is largely a result of structural forces, not just individual actions. A shared awareness of its origins could foster greater support for interventions that allow people to make healthier choices.
People and institutions need to work together to make healthy foods more accessible, affordable, appetizing, and convenient than unhealthy foods. Reversing the obesity crisis will require environments that promote physical activity and social movements that encourage people to get more exercise. We need to devote more resources to preventive efforts for all ages to improve our health.
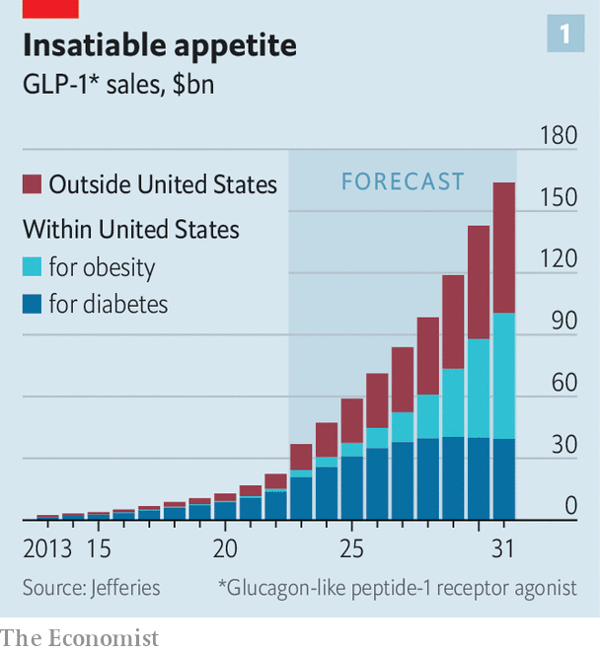
To reverse the obesity crisis, we will need an all-hands-on-deck approach. Pharmacological advances, surgery, and other treatments should complement new policies, societal practices, and population-wide interventions that promote healthier diets and decrease food consumption. Improving the nation’s health may require implementing policies perceived as restricting personal freedoms that have long been granted to industries and individuals. But these policies will be essential to keeping the population healthy.
For individuals, the goal should be to reach and maintain your optimum weight, meaning the weight at which your body the optimal physical and mental health.
Outline of free ebook:
INTRODUCTION: Struggling with Obesity
CHAPTER 1: How Do People Gain Excess Weight?
CHAPTER 2: Why Are People Getting Heavier?
CHAPTER 3: What Are the Consequences of Obesity?
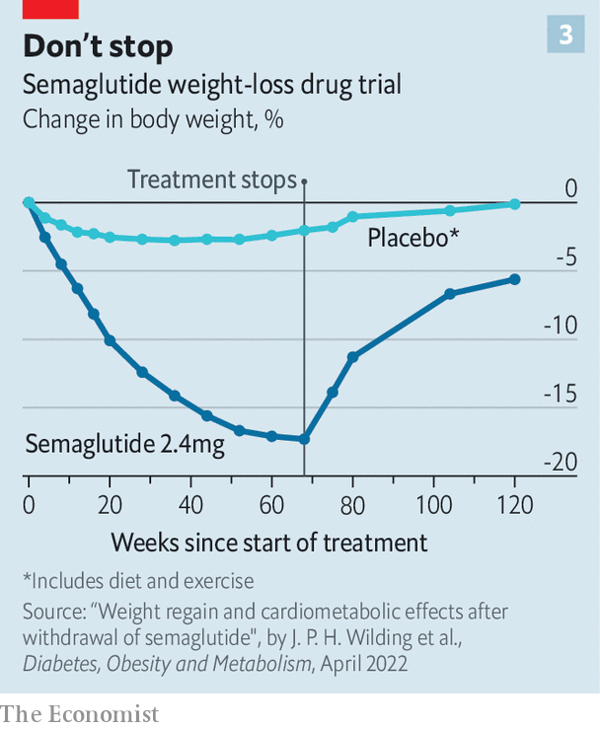
CHAPTER 4: What Are the Best Ways to Lose Weight?
CHAPTER 5: How to Reverse the Obesity Crisis