Banking on health: the world bank and health sector reform in Latin America

VALUES, ETHICS AND HEALTH CARE
Peter Duncan dixit:
We develop health care, and fund health care systems, broadly so that we can improve health. This very wide conception of the ends of health care leads us back to the kinds of things that Edwards mentions. From these, we can perhaps suggest that the values central to health care include things like autonomy (associated with further values such as free will, respect and consent), caring (also involving compassion and responsibility) and equality (which might also include values of justice and fairness).

A low incidence of catastrophic expenses sometimes reflects low service coverage (often in low-income countries) but sometimes occurs despite high service coverage (often in high-income countries). At a given level of service coverage, financial protection also varies. UHC index scores are generally higher in higher-income countries, but there are variations within income groups. Adjusting the UHC index for inequality in service coverage makes little difference in some countries, but reduces it by more than 10% in others. Seven of the 12 countries for which we were able to produce trend data have increased their UHC index over time (with the greatest average yearly increases seen in Ghana [1·43%], Indonesia [1·85%], and Vietnam [2·26%]), mostly by improving both financial protection and service coverage. Some increased their UHC index, despite reductions in financial protection, by substantially increasing their service coverage. The UHC index decreased in five of 12 countries with trend data, mostly because financial protection worsened with stagnant or declining service coverage. Our UHC indicators (except inpatient admissions) are significantly and positively associated with GDP per capita, and most are correlated with the share of health spending channelled through social health insurance and government schemes. However, associations of our UHC indicators with the share of GDP spent on health and the shares of health spending channelled through non-profit and private insurance are ambiguous.
Great article by Wagstaff and Neelsen.
Overcoming the Market Dominance of Hospitals
The facts:
Consolidation has been a predominant business strategy for hospitals and physicians in the United States for decades. Hospitals consolidate to gain market share and use resulting leverage to charge higher prices to private payers or employers large enough to self-insure. One major reason this may occur with relatively little resistance is the nature of health care markets. Numerous plans compete to offer health insurance to employers, and employers that self-insure must select from among these plans or third-party administrators (TPAs).
To attract employers, payers and TPAs strive to offer large networks of clinicians and health care centers to minimize care disruptions for employees. But when most physicians in a region are employed by a large hospital network, private payers and employers often have limited options other than to contract with that network, forcing them to tolerate 6% to 10% increases in prices each year.7 Adding to their leverage, these large networks often offer differentiated services like organ transplants or advanced specialty therapies that make them a “must-have” in private-payer or employer networks. Thus, the financial incentive for hospitals to merge or acquire physicians to gain must-have status is high.
Hospital consolidation is also supported by the nature of antitrust regulations, which are limited by how markets are defined. Since the 1990s, academics and regulators have defined local markets in health care using tertiary hospital catchment areas or hospital referral regions (HRRs). HRRs were constructed based on referral patterns of cardiovascular and neurosurgery hospitalizations from 1992-1993 Medicare data for research purposes.8 Yet these outdated HRRs meant for research are frequently used in antitrust enforcement today, despite the hospital mergers that have occurred since their development. In 2018, a review of community hospitals reported that 3491 of 5198 hospitals (67%) belonged to a multihospital health system, compared with just 2524 of 4956 (51%) in 1998.
Take-away message:
COVID-19 has the potential to exacerbate the nation’s history of hospital consolidation. Stronger incentives to counteract consolidation could protect patients against potential adverse effects of anticompetitive hospital networks. Policy makers and regulators should consider legislation that defines and regulates market-dominant hospitals MDHs, while promoting asset redistribution via market-dominant hospitals redistribution fund MRF, as a potential safeguard to the adverse consequences of the consolidation trend

HBR's 10 Must Reads on Platforms and Ecosystems
This collection of articles includes "Pipelines, Platforms, and the New Rules of Strategy," by Marshall W. Van Alstyne, Geoffrey G. Parker, and Sangeet Paul Choudary; "Strategies for Two-Sided Markets," Thomas R. Eisenmann, Geoffrey Parker, and Marshall W. Van Alstyne; "Finding the Platform in Your Product," by Andrei Hagiu and Elizabeth Altman; "What's Your Google Strategy?," by Andrei Hagiu and David B. Yoffie; "In the Ecosystem Economy, What's Your Strategy? ," by Michael G. Jacobides; "Right Tech, Wrong Time," by Ron Adner and Rahul Kapoor; "Managing Our Hub Economy," by Marco Iansiti and Karim R. Lakhani; "Why Some Platforms Thrive and Others Don't," by Feng Zhu and Marco Iansiti; "Spontaneous Deregulation," by Benjamin Edelman and Damien Geradin; "Alibaba and the Future of Business," by Ming Zeng; and "Fixing Discrimination in Online Marketplaces," by Ray Fisman and Michael Luca.
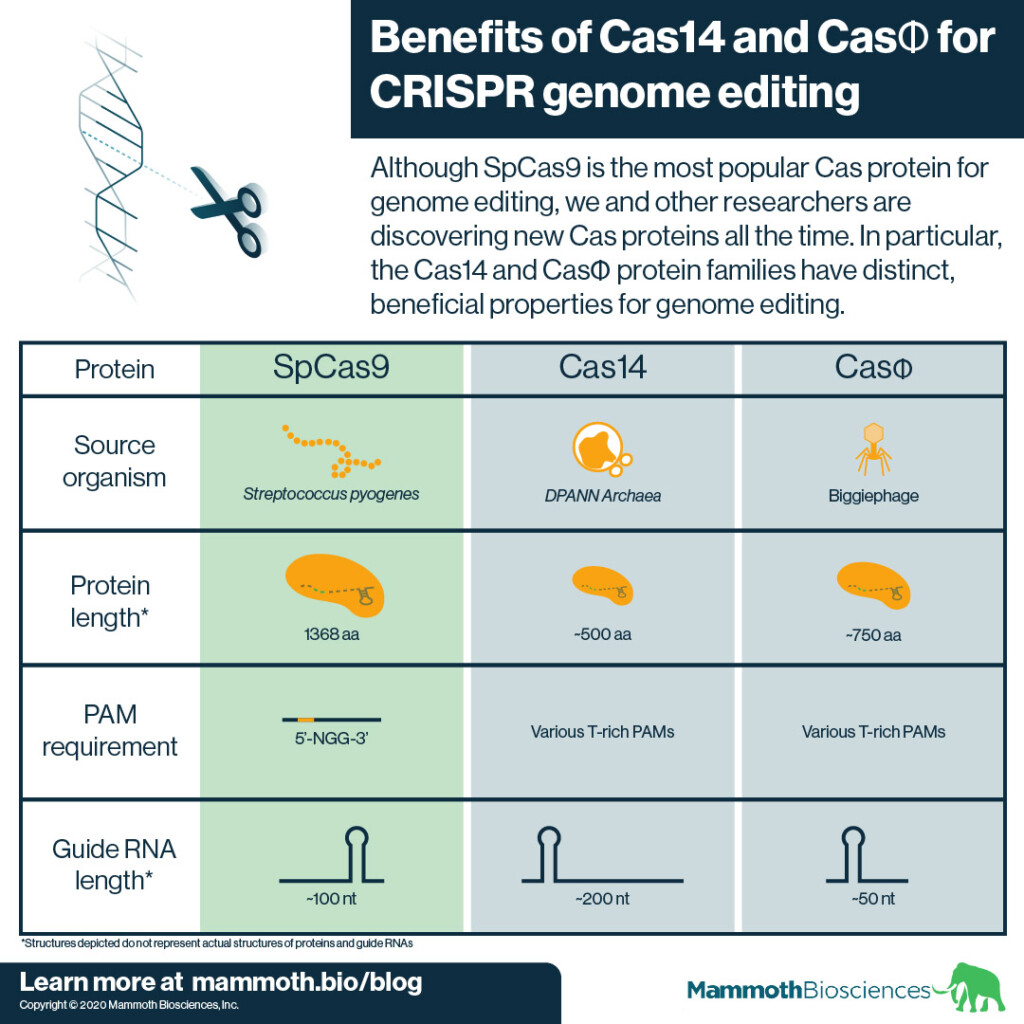
Expanding the possibilities of CRISPR genome editing with Cas14 and CasΦ
SpCas9 comes from a bacterium called Streptococcus pyogenes (hence “Sp”). S. pyogenes is a human pathogen. There is some evidence that using SpCas9 for genome editing in humans may lead to dangerous immune reactions (Ferdosi et al 2019) although other reports have questioned the importance of this finding.
In addition SpCas9 is quite large. It is 1368 amino acids (aa) long and can be difficult to fit into standard delivery vehicles (learn about CRISPR delivery here). Thus it can be hard to get SpCas9 into target cells and tissues.
Finally, SpCas9 requires the presence of a specific DNA sequence known as a “PAM” to target an adjacent sequence for genome editing. SpCas9’s PAM is 5’-NGG-3’. The need for this sequence restricts the number of sites SpCas9 can edit. This limits SpCas9’s usefulness.
Skills for the future health workforce: Preparing health professionals for people centred care
This is the focus of the OECD paper:
This paper discusses transversal (core) skills that are required by health professionals for a successful transition from fragmented and disease-centred care towards people-centred healthcare delivery systems. The discussion is motivated by the growing evidence of skills mismatch among health professionals. These transversal skills include interpersonal skills, such as person-centred communication, interprofessional teamwork, self-awareness and socio-cultural sensitivity, as well as analytical skills, such as adaptive problem solving to devise customised care for individual persons, system thinking, openness to continuous learning, and the ability to use digital technologies effectively
Sounds of interest. However, it forgets a key issue. Life sciences are changing and knowledge breaks barriers that gave birth to excessive specialization. Therefore, more issues to add in the next future.

Opportunities and challenges in long-read sequencing data analysis
Long reads: their purpose and place
Long-read sequencing, or third-generation sequencing, offers a number of advantages over short-read sequencing. While short-read sequencers such as Illumina’s NovaSeq, HiSeq, NextSeq, and MiSeq instruments; BGI’sMGISEQand BGISEQmodels; or ThermoFisher’s Ion Torrent sequencers produce reads of up to 600 bases, long-read sequencing technologies routinely generate reads in excess of 10 kb
Long-read technologies are improving rapidly, and may become the mainstay of sequencing; however, the broader application of long-read technologies are currently limited by a lower throughput, higher error rate and higher cost per base relative to short read sequencing. Wider use of such technologies in the clinical context may rapidly improve our understanding of cancer, pathogen evolution, drug resistance and genetic diversity in complex regions of the genome that have important implications for clinical care. Parallel development of existing technology to allow high throughput PCR-free sequencing will be important in sequencing difficult regions of the genome.
At present, no single long-read technology has any clear advantage from a scientific point of view, and thus it seems likely that the future of long-read sequencing is more likely to be decided on commercial terms rather than scientific. Whichever technology captures the market, it is clear that as these technologies become more affordable they will continue to shine a light into previously intractable regions of the genome with ever larger sample sizes and longer read-lengths, allowing new discovery in these evolving fields.
Just looking at stock exchange you may confirm that the decision is being made in commercial terms. It seems that there is a role for a cost-effectiveness evaluation right now.

Robert Frank, València 1952
Mort amb recepta (catalan version)
Annual report on Drugs in Catalonia (p.152)
Oxicodone in Catalonia: from 879.775 DDD in 2014 to 1.003.355 in 2019, a 14% increase. Tramadol: from 11.790.547 DDD in 2014 to 17.038.936 in 2019, a 69% INCREASE in 5 YEARS (p.152)
Daily Dose per Inhabitant (DDH)Tramadol: from 4,27 to 6,16 a 44,2% INCREASE in 5 YEARS
A worrying french situation
The documentary: Etats-Unis, la mort sur ordonnance
Nan Goldin denounces: Who profits form the opioid crisis?

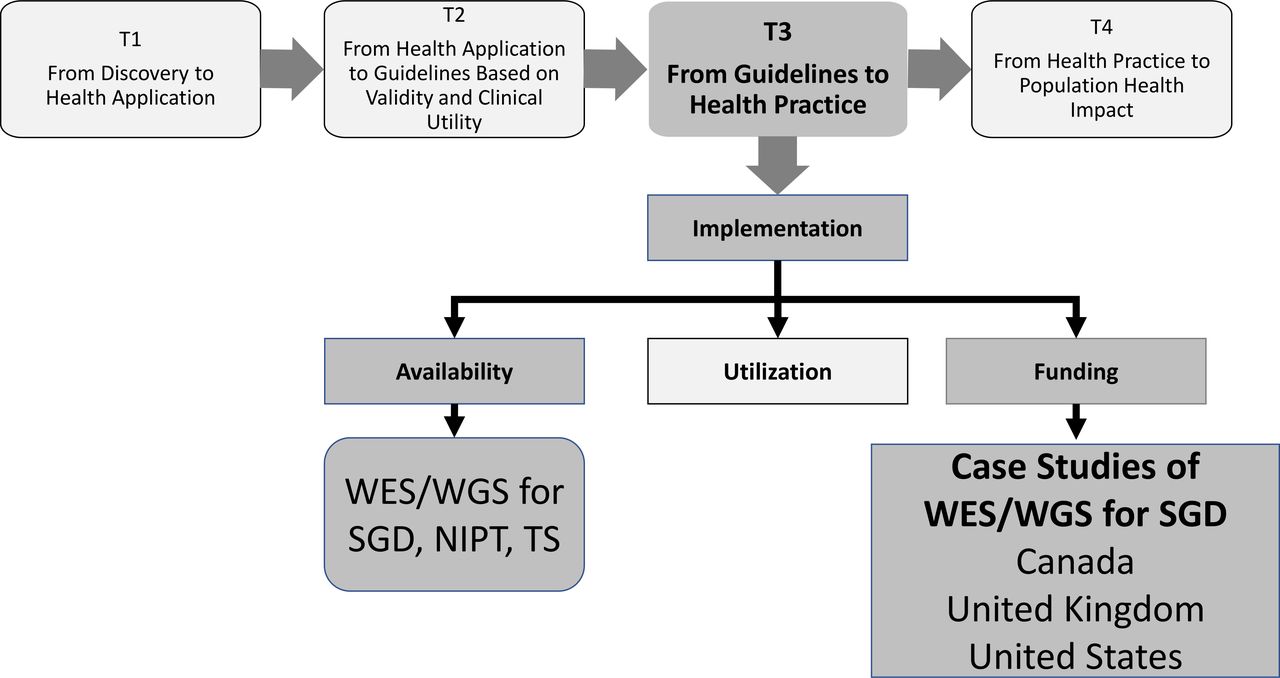
Availability and funding of clinical genomic sequencing globally
A useful review on the current situation:
Our case studies, based on published and unpublished literature as well as discussions with key experts in each country, are illustrative of three types of funding systems:
Publicly funded/national system: UK, which is one of a few countries with national, government-based funding for NGS (others include Belgium, Denmark, the Netherlands and Australia).
Publicly funded/provincial system: Canada, for which public funding of tests is provided at the provincial level after approval based on meeting specific criteria.
Mixed private/public system: USA, which has variable private and public insurer coverage.
The 4 steps:
Invent and Wander: The Collected Writings of Jeff Bezos
We believe that a fundamental measure of our success will be the shareholder value we create over the long term. This value will be a direct result of our ability to extend and solidify our current market leadership position. The stronger our market leadership, the more powerful our economic model. Market leadership can translate directly to higher revenue, higher profitability, greater capital velocity, and correspondingly stronger returns on invested capital.
(1997, Shareholder letter)

LOBBYING FOR CHANGE . Find Your Voice to Create a Better Society
Great questions and answers, by Alberto Alemanno:
How do we make government work for us? How can we save us from ourselves?
We face a dramatic gap between the problem-solving ability of our political system and our needs as a society. While this gap explains much of our social disengagement and disillusionment with traditional politics, it opens up a promising space for new, unconventional forms of active citizenship and civic engagement, as well as individual and collective empowerment.
This is the space we want and can occupy, as citizens. And it is set to grow as people abandon mainstream politics. That’s the space I want to you show you in the second part of this book.

The Plague Cycle. The Unending War Between Humanity and Infectious Disease
Take away conclusion:
In the Bible’s Book of Revelations, the Four Horsemen of the Apocalypse are sent forth to “kill with sword and with famine and with pestilence and by wild beasts,” and carry off a quarter of the earth. The identities of the horsemen are a matter of some debate: the fevered poetry is hard to decipher. While the Fourth Horseman seems to be Death himself, the Third Horseman is universally recognized as famine, and the Second as war, argument rages over the identity of the First Horseman: some recent experts suggest he is pestilence, others argue that he is Jesus Christ or the embodiment of righteousness.
It’s ironic that pestilence occupies the disputed saddle, for while throughout most of history violence and famine were two of Death’s most useful tools, the only one of the three that has ever managed to carry off a quarter of the earth at one go is pestilence. Plague ended the age of antiquity and ushered in the Renaissance. Infection shaped the age of global empires, and its decline boosted the economy of the modern world. Neither violence nor famine can claim to be its equal.
The frequency of violence, pestilence, and famine combined is why the idea that a good life should be one free of tragedy was mocked as utopian until the Industrial Revolution. They are the tools that nature used to keep humans in Malthusian misery. And none—famine, violence, or pestilence—has nearly the grip on humanity that it had even fifty years ago. A huge part of that progress is due to the fight against infection, flattening the plague cycle, and their knock-on effects.
The extent of disease has always shaped economic and social relations. Pandemics from centuries ago still help determine wealth and poverty, democracy and autocracy to this day. But the last half century clearly demonstrates that not all trends are inexorable. We’ve seen a massive global improvement in the quality of life even in parts of the world that suffered the most from the arrows of the First Horseman through the last two thousand years. Malthusian fatalism had a declining empirical basis in the nineteenth century. Now it has no basis at all.

The Billion-Dollar Molecule. The Quest for the Perfect Drug
On the business of science, and about the Vertex pharmaceutical firm and its IPO.
Aquí teniu un resum detallat de cada capítol del llibre "The Billion Dollar Molecule: One Company’s Quest for the Perfect Drug", basat en IA:
PART ONE: THE STORY
Chapter One: Aquest capítol, titulat "Squatting between the twin towers of the World Trade Center in New York City", descriu un "mercat de la carn" on diverses companyies presenten les seves necessitats financeres. Joshua Boger, que més tard fundaria Vertex, hi assisteix i ho descriu com un esdeveniment singular, subratllant la seva percepció de la baixa qualitat i desesperació de les presentacions. El capítol estableix l'ambient de la recerca de finançament en la indústria biotecnològica a principis dels anys noranta.
Chapter Two: Aquest capítol se situa a Cambridge, Massachusetts, un lloc amb una rica història educativa, especialment per la presència de Harvard. El capítol descriu els inicis de Vertex en un edifici en construcció, amb pols de ciment i canonades sense connectar, contrastant amb el tracte més luxós que els investigadors visitants havien rebut anteriorment a companyies com Merck. S'introdueixen figures clau com Stuart Schreiber de Harvard i Matt Harding de Yale, recentment contractat per Boger. El capítol també menciona la idea inicial de Boger de la implicació del Consell Assessor Científic (SAB), que no era popular dins de la companyia. Es planteja la qüestió de com obtenir avantatge en la investigació, comparant-ho amb entendre el funcionament d'un cilindre d'una pany.
Chapter Three: Aquest capítol es desenvolupa a la Universitat de Barcelona, durant una conferència científica on Thomas Starzl presenta resultats "impressionants" i "inversemblants" sobre el fàrmac FK-506. La sala s'omple amb uns 500 investigadors amb una "rara sensació d'anticipació". Starzl, tot i que es manté en segon pla, és la figura central, amb vint-i-sis dels trenta-un articles presentats provinents del seu grup. Només un d'aquests articles s'havia publicat prèviament a The Lancet. Es destaca la potència de FK-506 en comparació amb la ciclosporina.
Chapter Four: Aquest capítol continua a la mateixa conferència de Barcelona, centrant-se en la presentació de Takenori Ochiai de la Universitat de Chiba sobre un nou compost, també anomenat FK-506, que actua de manera similar a la ciclosporina en alentir la proliferació de cèl·lules T. La seva petita sala de presentacions s'omple "fins a vessar" amb figures destacades com Borel i Calne. Això crea un context de competència i interès en nous fàrmacs immunosupressors.
Chapter Five: Aquest capítol se centra en la tasca de John Thomson a Vertex, intentant aïllar proteïnes, específicament la FKBP bovina. Descriu el procés "laboriós" d'eliminació de fats i ceres mitjançant solvents orgànics, i com el propi proteïna també podia dissoldre's. Thomson treballa "dia i nit" en la sala freda, rentant i rentant l'extracte fins que gairebé és clar. A mesura que l'esforç s'amplia, Thomson comença a quedar-se a Vertex durant períodes cada vegada més llargs.
Chapter Six: Aquest capítol explora les negociacions de llicències entre Vertex i Harvard pel treball de Stuart Schreiber sobre la FKBP. Alec Behrakis de Harvard negocia amb Josh Boger de Vertex, advertint-lo que qualsevol menció accidental en una reunió del SAB podria obligar Vertex a pagar royalties elevats a la universitat, donant a Harvard un "dret de retenció" sobre la companyia. El capítol també subratlla l'amenaça que representen la personalitat i l'ambició de Schreiber, a qui li agrada parlar de si mateix i de les seves idees. La preocupació de Vertex no és que Schreiber trobi un compost competidor, sinó que els seus compostos siguin "exactament els mateixos". Es discuteixen estratègies per seguir a Schreiber i la seva manca de documentació.
Chapter Seven: Aquest capítol continua amb les interaccions amb Stuart Schreiber, revelant una oferta de Chugai Pharmaceutical per finançar la seva recerca a Harvard a canvi d'accés exclusiu a les seves troballes. Boger viatja a Nova York per reunir-se amb Nagayama de Chugai, presentant una diapositiva estàndard amb poca informació detallada. Tot i que Boger no menciona Schreiber, Nagayama sí que ho fa, oferint 40 milions de dòlars per la llicència, malgrat que Schreiber, el seu principal actiu, ara es considera "persona non grata" i possiblement un agent doble. Nagayama es retira a Tòquio sense comprometre's més enllà d'una nota.
Chapter Eight: Aquest capítol descriu la intensa feina dels científics de Vertex, inclòs John Thomson, abans de la visita de Glaxo. Boger es mostra "cranelike i immòbil", fixant la pantalla de l'ordinador. El capítol també menciona altres companyies petites que treballen en immunosupressió, com Cytel, que havia signat un acord amb Sandoz, cosa que obliga Boger a tenir-les en compte malgrat el seu menyspreu. Boger es prepara per a la reunió amb Glaxo, decidit a adaptar la seva presentació per persuadir-los del valor de la seva recerca, independentment dels seus interessos inicials.
Chapter Nine: Aquest capítol narra la reunió entre Vertex i Glaxo. Els executius de Glaxo mostren un gran interès, amb alguns prenent notes "furiósament". Debra Peattie de Vertex suggereix una manera de millorar l'ús de FKBP per seleccionar compostos, basada en una observació no publicada, fet que causa sorpresa i preocupació a Rich Aldrich. Peattie immediatament torna al laboratori per documentar la idea. Hudson de Glaxo es mostra entusiasta amb la mostra de FKBP bovina pura de Thomson i amb la revelació de Manual Navia d'haver obtingut els primers cristalls de la proteïna. Navia anomena els cristalls "Mickey Mouse" en privat.
Chapter Ten: Aquest capítol explora la complexa relació de Boger amb la ciència i el negoci, i la seva determinació de trobar el soci "òptim" per a Vertex, fins i tot si això significa cedir control i associar-se amb companyies que menyspreen la seva filosofia. S'introdueix Manuel Navia, un científic famós de Merck contractat per Vertex, la qual cosa va ser un "cop d'efecte" per a Boger, però que va causar ressentiment entre alguns dels altres científics. El capítol sembla reflexionar sobre les tensions entre la recerca científica pura i les necessitats empresarials d'una companyia biotecnològica emergent.
PART TWO: THE CHASE
Chapter Thirteen: Aquest capítol descriu les tres modes de funcionament de Vertex: projecte, protoprojecte i "preprotoprojecte". La investigació d'immunofilines havia estat en mode de projecte complet des del principi per necessitat. Tot i les "grans deficiències", com la incertesa sobre si Vertex tenia el "objectiu correcte", es van ignorar perquè Boger necessitava identificar ràpidament un camp on pogués afirmar tenir un avantatge. Des del punt de vista empresarial, l'estratègia va funcionar i Boger va poder vendre el projecte a un preu elevat. El capítol també menciona l'interès de Boger en les aspartil proteases, incloent la renina i la proteasa del VIH, cosa que el porta a una conferència a San Francisco. Les reunions del consell de projecte de Vertex, inclosa una sobre el VIH, es descriuen com a reunions a porta tancada amb científics vestits de manera informal.
Chapter Sixteen: Aquest capítol comença amb la descripció de com Stuart Schreiber estava planejant començar a tallar "senglars" després de la primera reunió del SAB. També es menciona la seva declaració humorística sobre una "malaltia rara" anomenada "timofília" i la seva suposada cura. Més tard, el capítol descriu com Manuel Navia observa Yamashita teclejant al laboratori. Els cristal·lògrafs normalment resolen l'estructura d'una proteïna un cop tenen un cristall prou gran, però necessiten verificar si realment han cristal·litzat proteïna. Yamashita havia intentat això la nit anterior, inserint un cristall en un tub capil·lar segellat i muntant-lo a l'aparell de raigs X de Vertex. L'aparell ocupa un terç del laboratori. Navia li pregunta a Yamashita si creu que han obtingut la "proteïna desitjada". Més tard aquella nit, Yamashita està desanimat a la sala de conferències, mentre Navia estudia a la biblioteca. Es descriu la ciència com una "fraternitat de dolor", particularment implacable amb el fracàs. Navia sent la necessitat de parlar amb Yamashita, tot i que prefereix no fer-ho.
Chapter Seventeen: Aquest capítol descriu una reunió sorpresa on Josh Boger anuncia la carta d'intencions entre Vertex i Chugai. Boger mostra un document amb la seva signatura i la de Nagayama, i després revela que és una carta d'intencions. Molts dels científics no entenen inicialment què estan veient. Boger ràpidament mostra una segona transparència titulada "L'Estàndard", que descriu l'acord de recerca entre Cytel i Sandoz. Aquest acord, que va aportar 30 milions de dòlars a Cytel però va garantir a Sandoz tots els drets sobre un fàrmac i el 30% de les accions de Cytel, es va considerar un rècord per a companyies petites. Boger murmura "Patètic" en comparació amb l'acord de Vertex.
Chapter Eighteen: Aquest capítol se centra en les negociacions entre Vertex i Chugai, amb Rich Aldrich enviant diàriament nombrosos memoràndums de diverses pàgines al Japó, que Boger anomena "granades". Aldrich treballa intensament per refinar les demandes de Vertex i les envia per fax abans d'anar al gimnàs. Els advocats i la gent de llicències de Chugai a Tòquio responen immediatament, mentre Aldrich fa exercici o intenta dormir. El capítol il·lustra la tensió i la intensitat de les negociacions internacionals en la indústria farmacèutica.
Chapter Nineteen: Aquest capítol canvia el focus a Thomas Starzl i la seva clínica de trasplantaments a Pittsburgh. La clínica es descriu com un lloc amb "magnífiques aspiracions" i el "grit i la commoció" d'una sala d'emergències d'una ciutat interior, realitzant fins a quinze trasplantaments per setmana. Starzl és la figura dominant, i FK-506 és el fàrmac clau. Després de la conferència de Barcelona, Starzl es va veure assetjat per peticions del fàrmac.
Chapter Twenty: Aquest capítol torna a Joshua Boger i la seva formació. A principis dels anys setanta, una excursió a un centre de ciències va tenir un gran impacte en ell. A novè grau, passava vint hores a la setmana programant al laboratori d'informàtica de la Fairfield University, on va estudiar química. Després va anar a la facultat de postgrau a Yale, on es va interessar per la vida molecular dels fàrmacs a mig camí de la seva tesi.

How New Models Of Vaccine Development For COVID-19 Have Helped Address An Epic Public Health Crisis
This acceleration has largely been fueled by an influx of resources—both financial and human—that is likewise record-setting. Significant levels of cooperation and innovation, which enable more-efficient use of those resources, have also played a key role.
There may be additional opportunities for innovation that deserve exploration. For example, master protocols, in which multiple vaccine or drug candidates are tested against a single control arm, could further accelerate clinical trials without compromising safety. Innovations to overcome potential delivery impediments, including supply chain challenges and insufficient numbers of health care workers in some regions, would also be welcome.
If widespread COVID-19 vaccination is realized in the coming months and years, the approach undertaken to arrive at that point will offer lessons for how to optimize the development and accessibility of vaccines against other pathogens, under both outbreak and non-outbreak scenarios. Our experiences with COVID-19 may also offer knowledge spillovers to other areas of medicine and public health.
More details in this Health Affairs issue.
Government, Big Pharma, and The People. A Century of Dis-Ease
A book to read, with this Table of Contents:

White Market Drugs. BIG PHARMA AND THE HIDDEN HISTORY OF ADDICTION IN AMERICA
A book to understand the contribution to addiction over a century.
By showing how the twenty-first-century opioid crisis is only the most recent in a long history of similar crises of addiction to pharmaceuticals, Herzberg forces us to rethink our most basic ideas about drug policy and addiction itself—ideas that have been failing us catastrophically for over a century.
This is the outline:
Introduction
Complicated legacies: The human genome at 20
On genome and precision medicine:
Debates about precision medicine (PM), which uses genetic information to target interventions, commonly focus on whether we can “afford” PM (17), but focusing only on affordability, not also value, risks rejecting technologies that might make health care more efficient. Affordability is a question of whether we can pay for an intervention given its impact on budgets, whereas value can be measured by the health outcomes achieved per dollar spent for an intervention. Ideally, a PM intervention both saves money and improves outcomes; however, most health care interventions produce better outcomes at higher cost, and PM is no exception. By better distinguishing affordability and value, and by considering how we can address both, we can further the agenda of achieving affordable and valuable PM.
The literature has generally not shown that PM is unaffordable or of low value; however, it has also not shown that PM is a panacea for reducing health care expenditures or always results in high-value care (17). Understanding PM affordability and value requires evidence on total costs and outcomes as well as potential cost offsets, but these data are difficult to capture because costs often occur up front while beneficial outcomes accrue over time (18). Also, PM could result in substantial downstream implications because of follow-up interventions, not only for patients but also for family members who may have inherited the same genetic condition. Emerging PM tests could be used for screening large populations and could include genome sequencing of all newborns, liquid biopsy testing to screen for cancers in routine primary care visits, and predictive testing for Alzheimer's disease in adults. These interventions may provide large benefits, but they are likely to require large up-front expenditures.

Now that Jeff Bezos anounces that he is to step aside as CEO, a summary in one figure:

The history, in one book:
Breast Cancer Risk Genes — Association Analysis in More than 113,000 Women
Genetic testing for breast cancer susceptibility is widely used, but for many genes, evidence of an association with breast cancer is weak, underlying risk estimates are imprecise, and reliable subtype-specific risk estimates are lacking.
However,
We found strong evidence of an association with breast cancer risk (Bayesian false-discovery probability, <0.05) for protein-truncating variants in 9 genes, with a P value of less than 0.0001 for 5 genes (ATM, BRCA1, BRCA2, CHEK2, and PALB2) and a P value of less than 0.05 for the other 4 genes (BARD1, RAD51C, RAD51D, and TP53).
None of the other 25 genes in the panel had a Bayesian false-discovery probability of less than 0.10. Of note, 19 genes had an upper limit of the 95% confidence interval of the odds ratio of less than 2.0, with 2.0 representing a proposed threshold for “pathogenic, moderate risk alleles”9; we therefore conclude that these genes are not informative for the prediction of breast cancer risk. We confirmed that missense variants in BRCA1, BRCA2, and TP53 that would be classified as pathogenic according to clinical guidelines are indeed associated with clinically significant risks. We also found that rare missense variants in CHEK2 overall, as well as variants in specific domains in ATM, are associated with moderate risk.
The summary:
Variants in 8 genes — BRCA1, BRCA2, PALB2, BARD1, RAD51C, RAD51D, ATM, and CHEK2 — had a significant association with breast cancer risk.

Biotechnology in the Time of COVID-19
Our journey is far from over. In my mind, it is our responsibility as an industry, as a company, and as global citizens to help ensure a pandemic of this magnitude never happens again. I’ve worked in infectious diseases for my entire career—and I’ve been exposed to the disruption, the health crises, and the economic fallout they create. It is up to all of us to bring forward solutions. I hope you will join the many companies, worldwide health agencies, and nongovernmental organizations that are answering the call. Together, we can all use our skills to help serve people in this remarkably urgent time of need.
Great words by Stephane Bancel, CEO of Moderna

Recent evolutions of machine learning applications in clinical laboratory medicine
You'll find an interesting review about laboratory medicina and machine learning in this article, with applicatons to chemical chemistry, hematology and microbiology.
There has been a recent rise in various ML applications in the field of clinical laboratory medicine. Despite the potential of ML to ameliorate the efficiency of laboratory processes and optimize diagnostic workflows, translation into routine practice is still slow-going. There is a need to raise more awareness about the vast ML landscape among laboratory professionals. Educational programs dealing with theoretical ML concepts as well as their associated challenges and opportunities could stimulate wider acceptance and exploitation in the clinical laboratory. It is important to realize that ML will not immediately function as a surrogate of the laboratory professional’s neural networks, but will rather act as a valuable supportive tool with the capability of increasing the odds on optimal outcomes for patients accessing health care.
Margaret Huntington Boehner
The Great Risk Shift. The New Economic Insecurity and the Decline of the American Dream