The dark side of the force
While reading today FM Alvaro op-ed on current war:
Questions in a war, I thought that was good to remember
Jack Hirshleifer and specifically to retrieve an excellent speech he gave in 1993:
The dark side of the force. When I read it for the first time I got impressed and I've remembered forever.
Therefore, my suggestion is to read the whole speech. If you are an economist, you'll be shaken by his views. Selected statements:
“Our profession has on the whole taken not too harsh but rather too benign a view of the human enterprise. Recognizing the force of self-interest, the mainline Marshallian tradition has nevertheless almost entirely overlooked what I will call the dark side of the force—to wit, crime, war, and politics."
“cooperation, with a few obvious exceptions, occurs only in the shadow of conflict.” “when people cooperate, it is generally a conspiracy for aggression against others (or, at least, is a response to such aggression).”
"Pareto is saying, sure, you can produce goods for the purpose of mutually beneficial exchange with other parties—OK, that's Marshall's "ordinary business." But there's another way to get rich: you can grab goods that someone else has produced. Appropriating, grabbing, confiscating what you want— and, on the flip side, defending, protecting, sequestering what you already have—that's economic activity too. Take television. Cops chase robbers, victims are stalked by hitmen (or should I say hitpersons?), posses cut off rustlers at the pass, plaintiffs sue defendants, exorcists cast spells against vampires. What is all this but muscular economics? Robbers, rustlers, hitpersons, litigants—they're all trying to make a living. Even vampires are making economic choices: sucking blood is presumably the cost-effective way of meeting their unusual nutritional needs.”
“This is Machiavelli's version of the golden rule: he who gets to rule, will get the gold. Human history is a record of the tension between the way of Niccolo Machiavelli and what might be called the way of Ronald Coase. According to Coase's Theorem, people will never pass up an opportunity to cooperate by means of mutually advantageous exchange. What might be called Machiavelli’s Theorem states that no one will ever pass up an opportunity to gain a one-sided advantage by exploiting another party.
Machiavelli's Theorem standing alone is only a partial truth, but so is Coase's Theorem standing alone. Our textbooks need to deal with both modes of economic activity. They should be saying that decision-makers will strike an optimal balance between the way of Coase and the way of Machiavelli—between the way of production combined with mutually advantageous exchange, and the dark-side way of confiscation, exploitation, and conflict.”
"Thus, in recognizing the role of conflict we must not go overboard in the other direction. All aspects of human life are responses not to conflict alone, but to the interaction of the two great life-strategy options: on the one hand production and exchange, on the other hand appropriation and defense against appropriation. Economics has done a great job in dealing with the way of Ronald Coase; what we need now is an equally subtle and structured analysis of the dark side: the way of Niccolo Machiavelli.”
The balance between these modes of economic activity--the one leading to greater aggregate wealth, and the other to conflict over who gets the wealth--provides the main story line of human history.
This speech and several articles on conflict were published in a book "
The Dark Side of the Force: Economic Foundations of Conflict Theory".
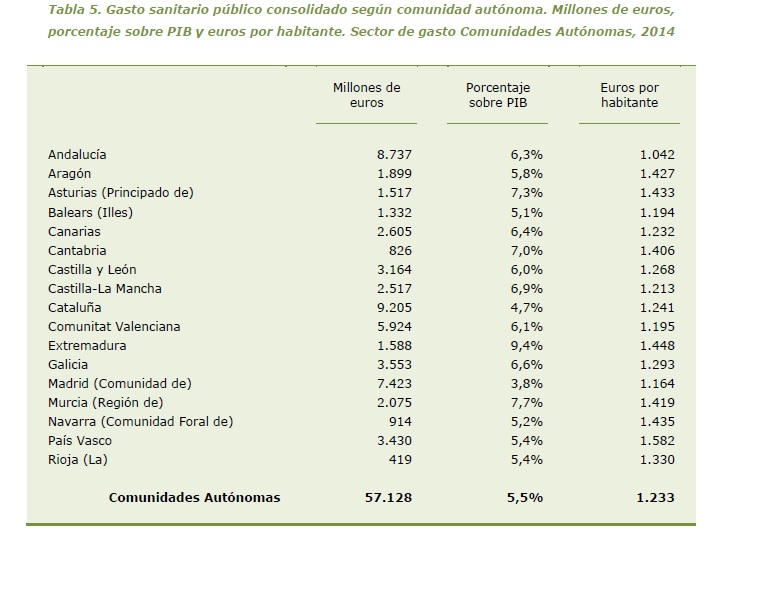
Hirshleifer analytic frame may be applied to health economics as well, specifically to such cases where fraud, inappropriateness, and false advertising are part of the dark force.
PS. Long time ago
I quoted in a post the Schelling book on the same topic.