What's on the horizon for bioethics?
The Nuffield Council of Bioethics released a short overview of current critical issues. It is really helpful.
What's on the horizon for bioethics?
The Nuffield Council of Bioethics released a short overview of current critical issues. It is really helpful.
Adam Wagstaff laid out a strong case against labor-tax financing for health insurance,based on analyses of the potential revenue generation, the distributional implications, the impact on the labor market, and the potential for universality in service coverage
A key problem with labor-tax social health insurance is that it can actually redistribute resources toward the wealthy, not the poor. This occurs when general revenues subsidize labor-tax social health insurance institutions that predominantly serve upper-income groups instead of having those subsidies be used to extend coverage to the rest of the population. When expenditures on health care for the eligible workers in the formal sector—already higher than expenditures for the general population—exceed their contributions, the resulting subsidy is financed through taxes levied on the entire population (for example,value-added taxes), which is a form of upward redistribution.

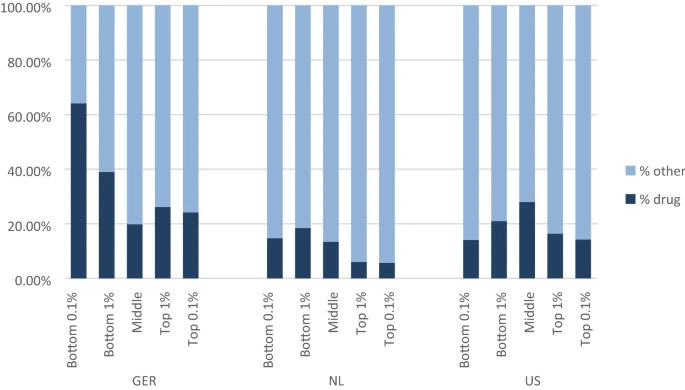
The high degree of persistence in membership in the extremes of the residual spending distribution in all three countries raises concerns that insurers might take steps to deter those who tend to be underpaid and attract those who tend to be overpaid. Attracting the healthy/deterring the sick among subsets of the populations with the disease indicators (such as diabetes) prevalent on both extremes of the residual spending distribution could be a highly profitable strategy, and potentially lead to distortions in the efficient care for these groups. In response to these findings, we proposed a form of reinsurance, based on residuals, and targeted to members of a “risk pool” defined on past-year very high undercompensation. Careful targeting (along with re-estimating the beta weights in risk adjustment to take into account the reinsurance payments) leads to very substantial improvements in overall fit of payments to spending, with especially large effects for the most extremely under- and overcompensated. The share of people affected by this form of risk sharing is very small, less than 3 in 1000 in all three countries. While our proposed policy seems effective in better tying payments to spending, there are alternative approaches to the same issue. One example would be to find ways to split groups like those with diabetes and other illnesses prevalent among the undercompensated into those likely to be on one or the other side of the residual spending distribution. Calling attention to the powerful effects members of the tails of the residual distribution have on the overall fit of the models is the first step in directing policy attention to these important groups.
Revisiting Compression of Morbidity and Health Disparities in the 21st Century
Age, Socioeconomic Status, and Health
Compression of morbidity:
an ideal population health dynamic in which people live long, healthy lives with declines in physical and cognitive health associated with senescence “compressed” into a short time period at the end of life.
There are many ongoing debates in the compression of morbidity literature, including which measures of morbidity should be prioritized and the best methodological approaches for life course analyses that adequately address the thorny challenge of isolating age, period, and cohort effects. Even so, the extant research literature regarding compression of morbidity in the United States suggests that it is not happening at the population level.[3] However, much of the published research does not stratify analyses by socioeconomic position, as House and colleagues had recommended in 1990. House, Lantz, and Herd’s 2005 longitudinal analysis of ACL data affirmed that those in the highest income and education groups were significantly more likely to postpone physical functional impairments until much later in life

Too Much Information. Understanding What You Dont Want to Know
NYT created a weekly bulletin for those that only want to read good news. This means that they are not interested in what's going on really. Does this make sense? Cass Sunstein would say yes and in the book explains why.

In contrast to the political and policy emphasis placed upon ‘person focus’, there is continuing debate about its actual meaning in the health care context vis-à-vis concepts such as ‘patient-centred’, ‘user-centred’, ‘family-centred’ or ‘people-centred’ care, or indeed ‘personalized’ health care, as well as the strategies that are available and effective to promote and implement ‘person focus’. There is no single definition of related concepts, and there are different views on the extent to which patient or person-centredness.
This book precisely tries to shed some light on the issue:

