Some months ago I wrote a post on TMT syndrome. It raised the interest of some followers and I was asked to prepare a larger op-ed for a bulletin (in spanish):
El síndrome TMT ante la destrucción creativa
Hoy en día podemos conocer con precisión las preferencias de lectura en una revista electrónica; podemos identificar cuántos acceden a ella y así nos podemos aproximar a las preocupaciones de los lectores. Health Affairs es una revista de referencia en política y gestión sanitaria y, en el ranking de artículos leídos en 2013, la primera posición la ocupa una revisión sobre una asignatura pendiente: la adopción de las tecnologías de la información en el sector salud [1]. El artículo se pregunta si las tecnologías de la información en Estados Unidos están interconectadas, ampliamente implantadas, utilizadas adecuadamente y si se ha producido el cambio organizativo esperado. La respuesta a cada cuestión es simplemente negativa. Y como todo artículo que desea resumir algo complejo en cinco páginas y recurre a generalizaciones, la conclusión a la que llega es parcial. Porque hay una gran mayoría de tareas pendientes por hacer y también hay otras que ya se han hecho y fueron publicadas en el propio Health Affairs cuatro años antes, como es el caso, por ejemplo, de Kaiser Permanente [2]. La barrera fundamental a la adopción de la tecnología tiene que ver con la organización y los incentivos. Entornos de atención fragmentada y con pago por acto médico tienen todos los ingredientes necesarios para que la adopción de tecnologías de la información se deje para otro día.
La tecnología está disponible, la organización está llamada a prepararse para adoptarla, pero en muchos casos, los incentivos escasean. De lo mucho que hay escrito al respecto, me sigue interesando el libro que coordinó Louise Liang desde Kaiser Permanente [3]. En él, los protagonistas de la experiencia de implantación de la historia clínica electrónica describen su visión y las perspectivas de futuro. Los últimos capítulos interesan en especial. Cuando el uso de aplicaciones móviles parece que sea el próximo milagro para la salud [4], David Eddy y Louise Liang se olvidan de ello y se concentran en explicar la importancia de las trayectorias en enfermos crónicos y los modelos probabilísticos que hay detrás del “Archimedes Model”. Todo dirigido a un solo objetivo: mejorar la toma de decisiones compartidas entre médico y paciente. De este modo, llegan al núcleo esencial del valor potencial de las tecnologías de la información: mejorar las decisiones y mejorar el proceso de atención.
Estoy convencido que estamos en el sector salud ante el síndrome TMT (too much technology, demasiada tecnología). Las organizaciones son incapaces de digerir la transformación potencial que tiene implicaciones cruciales en el coste y en la calidad. Los requisitos para que esta transformación sea efectiva se han descrito en múltiples ocasiones y ahora, en un contexto económico de límites a la inversión, puede que haya una barrera adicional a la organizativa.
En nuestro entorno próximo, hay casos ejemplares de adopción de historia clínica electrónica. Hay organizaciones que desde hace más de una década disponen de información digitalizada completa de la población que atienden [5], del mismo modo que hay entornos donde escasean ejemplos similares, como sucede en la sanidad privada.
La cuestión emergente es dilucidar hasta qué punto la digitalización generalizada en el sector salud será capaz de modificar ampliamente la “función de producción” de la salud tal como la conocemos hasta ahora. Con ello quiero referirme fundamentalmente a la asistencia sanitaria y a los comportamientos saludables.
Eric Topol ha sido capaz de resumir en un libro lo que está sucediendo y lo que puede suceder [6]. Más allá de confirmar las tendencias conocidas y sus implicaciones, al final, cuando llega al capítulo sobre la necesaria “plasticidad de los médicos”, nos muestra el panorama al que las organizaciones, los profesionales y el regulador han de enfrentarse próximamente.
En el capítulo relativo al “homo digitus”, nos aporta su conclusión: “La especie humana está digitalizando la propia especie, este es el agente último de cambio de la vida. Y esto va más allá de un simple cambio, es la esencia de la destrucción creativa que conceptualizó Schumpeter”. ¿Seguiremos en medio del síndrome TMT o finalmente entraremos en un proceso de destrucción creativa? Si alguien os plantea este dilema, desconfiad del reduccionismo; estoy convencido que estamos en medio del proceso, aunque no podemos dilucidarlo.
Referencias
[1] Kellermann AL, Jones SS (2013). What it will take to achieve the as-yet-unfulfilled promises of health information technology. Health Affairs, 32(1):63-8.
[2] Chen C, Garrido T, Chock D, Okawa G, Liang L (2009). The Kaiser Permanente Electronic Health Record: transforming and streamlining modalities of care. Health Affairs, 28(2):323-33.
[3] Liang LL, ed. (2010). Connected for Health: Using Electronic Health Records to Transform Care Delivery. San Francisco CA: Jossey-Bass.
[4] The Economist (2014). Health and happiness. 1st February.
[5] Saigí F (2007). La informatització de la informació sanitària: projectes i experiències d’història clínica compartida. Vol. 1, Cap 4. En: Universitat Oberta de Catalunya, Generalitat de Catalunya. Projecte Internet Catalunya. Modernització tecnològica, canvi organitzatiu i serveis als usuaris en el sistema de salut de Catalunya. Barcelona: UOC.
[6] Topol E (2012). The Creative Destruction of Medicine: How the Digital Revolution Will Create Better Health Care. New York: Basic Books.
22 d’abril 2014
16 d’abril 2014
Is it possible to internalize externalities of risky behavior?
Risking Your Health. Causes, Consequences, and Interventions to Prevent Risky Behaviors
Behaviour Change
Today I bring a World Bank Report and a UK Parliament report, both on behaviour. The first is closely related to developing countries, though the same messages are for developed ones. I don't know who exactly is paying the bill for such risky behaviours. Measures to internalize externalities are not so easy to implement, though the document explains some of them.
The second report is an introduction to behavioral economics for politicians. I'm convinced that we do need to know more about this, although there is no unifying theory and prescriptions are fuzzy by now.
PS. Today we can confirm that Google scans your gmail messages.
PS. Today we can also confirm again that internet is an unsafe network
PS. Bloomberg on behavioral finance.
Behaviour Change
Today I bring a World Bank Report and a UK Parliament report, both on behaviour. The first is closely related to developing countries, though the same messages are for developed ones. I don't know who exactly is paying the bill for such risky behaviours. Measures to internalize externalities are not so easy to implement, though the document explains some of them.
The second report is an introduction to behavioral economics for politicians. I'm convinced that we do need to know more about this, although there is no unifying theory and prescriptions are fuzzy by now.
PS. Today we can confirm that Google scans your gmail messages.
PS. Today we can also confirm again that internet is an unsafe network
PS. Bloomberg on behavioral finance.
15 d’abril 2014
The home and the neighborhood
Transforming Specialty Practice — The Patient-Centered Medical Neighborhood
The coordination of health services requires intense relationships between primary and specialized care. Though this is obvious, sometimes there is a need to insist on it. And this is precisely what an article at NEJM does. It explains the components to assess the Patient centered medical home and the patient centered specialty practice.
This is a US style organizational design, although some european private organizations should keep an eye on such developments. The current organization of private practice is too far from the requirements of a modern practice of medicine and to fulfill patient expectations. The pressures for organizational change unfortunately will not arise from inside, the confort zone always plays its role.
PS. Video on low value care and how to avoid it, at NEJM.
The coordination of health services requires intense relationships between primary and specialized care. Though this is obvious, sometimes there is a need to insist on it. And this is precisely what an article at NEJM does. It explains the components to assess the Patient centered medical home and the patient centered specialty practice.
This is a US style organizational design, although some european private organizations should keep an eye on such developments. The current organization of private practice is too far from the requirements of a modern practice of medicine and to fulfill patient expectations. The pressures for organizational change unfortunately will not arise from inside, the confort zone always plays its role.
PS. Video on low value care and how to avoid it, at NEJM.
14 d’abril 2014
The Health of Catalans
La salut de la població de Catalunya en el context europeu
Comparing population health between countries allows to understand the scope of the differences. Some of them are unwarranted and others require an explanation. Anyway, it is good to confirm in a new report that the health of catalans has achieved a top level in Europe. The key indicator is healthy live years. As a summary it works, but when you go into details, then some problems arise: obesity, tobacco, colon cancer, diabetes,...
Comparing public expenditures , Catalonia spends less than other countries with similar GDP. And the opposite is true for private expenditures (p.16). Unfortunately, data is from 2010 and things have changed a lot, on GDP and health expenditure. My guess is that right now we are spending publicly a larger percentage than 6%. An update is needed in order to know better our current position.
Comparing population health between countries allows to understand the scope of the differences. Some of them are unwarranted and others require an explanation. Anyway, it is good to confirm in a new report that the health of catalans has achieved a top level in Europe. The key indicator is healthy live years. As a summary it works, but when you go into details, then some problems arise: obesity, tobacco, colon cancer, diabetes,...
Comparing public expenditures , Catalonia spends less than other countries with similar GDP. And the opposite is true for private expenditures (p.16). Unfortunately, data is from 2010 and things have changed a lot, on GDP and health expenditure. My guess is that right now we are spending publicly a larger percentage than 6%. An update is needed in order to know better our current position.
10 d’abril 2014
A pivotal moment in the history of medicine
What the Tamiflu saga tells us about drug trials and big pharma
Today the long article by Ben Goldacre published in The Guardian is a required reading. Those that have some doubts regarding the effectiveness of oseltamivir will see them vanishing. The Cochrane review explains the size of side effects and controversies that have surrounded such drug since flu pandemic in 2009.
The most important message goes beyond tamiflu, it is related to transparency in drug trials:
Today the long article by Ben Goldacre published in The Guardian is a required reading. Those that have some doubts regarding the effectiveness of oseltamivir will see them vanishing. The Cochrane review explains the size of side effects and controversies that have surrounded such drug since flu pandemic in 2009.
The most important message goes beyond tamiflu, it is related to transparency in drug trials:
This is a pivotal moment in the history of medicine. Trials transparency is finally on the agenda, and this may be our only opportunity to fix it in a decade. We cannot make informed decisions about which treatment is best while information about clinical trials is routinely and legally withheld from doctors, researchers, and patients. Anyone who stands in the way of transparency is exposing patients to avoidable harm. We need regulators, legislators, and professional bodies to demand full transparency. We need clear audit on what information is missing, and who is withholding it.
Finally, more than anything – because culture shift will be as powerful as legislation – we need to do something even more difficult. We need to praise, encourage, and support the companies and individuals who are beginning to do the right thing.
07 d’abril 2014

04 d’abril 2014
A primer on health economics and policy
Social values in health and social care
In just 38 pages Tony Culyer explains the basics of health policy. It is not a review, these are a collection of key insights that basically come from his book. This is the outline:
.
In just 38 pages Tony Culyer explains the basics of health policy. It is not a review, these are a collection of key insights that basically come from his book. This is the outline:
- Introduction
- Liberalism versus libertarianism
- The market versus the state
- Public versus private insurance
- Equity versus equality
- Inequalities of health versus inequalities of health care
- Equity versus efficiency
- Needs versus wants
- Prices versus rationing
- Financial protection versus quality of life
- Public versus private
- Agents versus principals
- Universality versus selectivity
- Comprehensiveness versus limited benefit bundles
- Centralisation versus decentralisation
- Competition versus collaboration
- Experts versus citizens
- Mixing values and other things
- Key messages
Cost is also a value and no mere matter of accountancy. If we introduce a newMany politicians don't want to hear such messages. I stronlgy suggest you to read this booklet from Kings' Fund.
health care procedure, the cost will have to come out of expenditure elsewhere
in the NHS –unless there is a concurrent increase in the NHS budget. But less
expenditure elsewhere will normally imply reduction of service elsewhere and
a consequential health loss. The true cost of getting more care (and hence
health) in one area of activity is therefore the minimum necessary loss of care
(and loss of health) elsewhere. This is the important notion of opportunity cost.
.
03 d’abril 2014
Cost-effectiveness as a proxy of value
GUIA I RECOMANACIONS PER A LA REALITZACIÓ I PRESENTACIÓ D'AVALUACIONS ECONÒMIQUES I ANÀLISIS D'IMPACTE PRESSUPOSTARI DE MEDICAMENTS EN L’ÀMBIT DEL CATSALUT
As resources are scarce we do have to prioritise. That's it, we can't escape. We do need a proxy to assess relative incremental value of the technologies and procedures for a disease, otherwise decisions would be arbitrary. In such situation a methodologic guide is welcome to provide credible information. This is precisely what the guide by CatSalut is contributing to. It explains criteria and ways to present economic evaluation and budget impact analysis. A well designed guide that unfortunately right now will have a limited application. The reason is that government can't completely decide about it. It's an issue of months.
As resources are scarce we do have to prioritise. That's it, we can't escape. We do need a proxy to assess relative incremental value of the technologies and procedures for a disease, otherwise decisions would be arbitrary. In such situation a methodologic guide is welcome to provide credible information. This is precisely what the guide by CatSalut is contributing to. It explains criteria and ways to present economic evaluation and budget impact analysis. A well designed guide that unfortunately right now will have a limited application. The reason is that government can't completely decide about it. It's an issue of months.
02 d’abril 2014
Unsafe medical devices regulation
Improving Medical Device Regulation: The United States and Europe in Perspective
The regulatory differences between Europe and US are quite well known since the breast implants scandal. A US citizen was not able to receive such implant because FDA had not approved. The rationale is not related to such a case, it is the current system of notified bodies that really doesn't protect population health. However, US needs also to improve. Milbank Quarterly article says:
PS. Milbank says it is an original investigation, you may check the same title and authors some months before in Value in Health
The regulatory differences between Europe and US are quite well known since the breast implants scandal. A US citizen was not able to receive such implant because FDA had not approved. The rationale is not related to such a case, it is the current system of notified bodies that really doesn't protect population health. However, US needs also to improve. Milbank Quarterly article says:
Overall, US and European evidence requirements for devices introduce not only risks to patients but also the wrong incentives to generate the needed evidence to better understand and evaluate the benefits and risks of new devices. Considering that manufacturers often take advantage of existing evidence from already marketed devices to gain approval for a new device, they are reluctant to undertake new clinical studies. In addition, because later devices may be able to claim equivalence, the first manufacturer to market does not have a very strong incentive to undertake extensive clinical studies.The steps to improve regulation are detailed in the article. Surprisingly, notified bodies is again the chosen option in the current review of the legislation. Citizens should know it before voting.
PS. Milbank says it is an original investigation, you may check the same title and authors some months before in Value in Health
01 d’abril 2014
The foundations of a Health Policy consensus
Last Friday in Parliament, a document reflecting the foundations of a health policy consensus was presented. As a coordinator I gave a short speech highlighting salient features of the agreement. This is what I said:
I'm really convinced about the relevance of such consensus. From now on, Parliament will have to achieve a final agreement among the parties. Let's wait for a successful closing.
PS. Afterwards I was interviewed at 8TV.

Molt Honorable Presidenta del Parlament de Catalunya, Honorable Conseller, Il.lustríssims diputats, autoritats i membres de la comissió.El fet que ens reuneix avui aquí és donar resposta a la Moció 3/X adoptada en aquest Parlament per la qual s’instava al Govern a lliurar un document de bases que definís com havia de configurar-se el Sistema Nacional de Salut . El Govern de la Generalitat va aprovar el 21 de maig passat la creació de la Comissió amb aquest objectiu formada per representats del grups parlamentaris i els membres del Consell Català de la Salut.
És per això doncs que venim a presentar-vos els resultats dels treballs que hem realitzat en aquests mesos i són la mostra d’un consens entorn de vuit àmbits clau del sistema públic de salut: el finançament i la cobertura, els professionals, les prestacions i el catàleg de serveis, el model de serveis, l’avaluació, rendiment de comptes i transparència, compromís ciutadà, recerca i innovació i governança.En cadascun d’ells hem mantingut un debat ampli i obert. Hem volgut concretar principis i criteris que cal respectar i tenir en compte. Hem evitat entrar en els instruments concrets que cal utilitzar per a dur-los a terme, en la mesura que vam considerar que corresponia als responsables polítics i gestors de cada moment. Hem tractat de fixar-nos en aquells aspectes que més preocupen a la ciutadania.
La salut es troba al capdamunt de les prioritats de tota persona i sabem que al costat de compromís individual convé que els poder públics siguin capaços de d’oferir respostes col·lectives per una millor salut poblacional. És en aquest sentit que voldria seleccionar i destacar algunes de les 83 propostes que es mostren al document.
En l’àmbit de Finançament i cobertura s’assenyala amb claredat l’opció per un accés universal de la ciutadania al Sistema Nacional de Salut i alhora s’estableix un criteri de nivell de finançament públic en salut suficient i sostenible, que es relacioni amb el nivell de riquesa del país i que convergeixi amb la despesa de països amb producte interior brut per càpita equivalent i sistema sanitari similar.
En l’àmbit dels professionals s’ha considerat que la planificació de necessitats de professionals, les competències i capacitats acreditades han de ser objecte reconsideració atenent als canvis sociodemògràfics, econòmics i tecnològics. S’explicita l’èmfasi en el professionalisme com a criteri que guia la relació entre professionals amb la ciutadania, amb el sistema sanitari i els proveïdors, i la necessitat d’establir mecanismes per tal de fer efectiva la participació dels professionals en l’elaboració de polítiques i la gestió.
En l’àmbit relatiu a prestacions, s’ha considerat que cal un catàleg bàsic que respecti els criteris de seguretat, evidència científica, cost-efectivitat i avaluació d’impacte pressupostari, que és rellevant tenir en compte tant l’atenció sanitària com les intervencions comunitàries de salut pública. La garantia d’equitat d’accés a les prestacions amb qualitat cal preservar-la davant tota necessitat de salut.
En l’àmbit de model de serveis es té en compte quins han de ser els elements clau, en primer lloc les estratègies de promoció, protecció de la salut i prevenció de la malaltia, integrar las salut pública i comunitària en el model assistencial. Es mostra la rellevància de l’accessibilitat, de la gestió de casos i de la integració assistencial, així com el reforç a l’atenció primària dotant-la de més capacitat resolutiva.
En aquest àmbit també s’explicita la necessitat de respectar un conjunt de criteris en la relació contractual entre el finançador i el proveïdor, com per exemple explicitar l’orientació als resultats de salut i qualitat assistencial, la transparència interna i externa dels contractes i resultats, i els incentius a l’eficiència. Es demana d’elaborar i aplicar una normativa reguladora de la provisió d’activitat privada en els centres del SISCAT que ha de contemplar un codi ètic, una regulació de preus de prestacions complementàries, i mecanismes de controls i transparència.
En l’àmbit sobre rendiment de comptes es mostren un conjunt de mesures per tal de fer efectiva la difusió d’informació que contribueixi a la generació de coneixement i millors presa de decisions.
En l’àmbit de compromís ciutadà es destaca el paper del ciutadà com agent actiu del sistema de salut, sobre la presa de decisions compartides en tots els processos de malaltia i en especial al final de la vida.
En l’àmbit de recerca s’assenyala la importància d’optimitzar els recurs i alhora promoure noves fonts de finançament per a projectes.
En l’àmbit de governança es revisen les funcions entre diferents organismes i les seves responsabilitats, el paper del Departament cm a responsable de les polítiques sanitàries, el Servei que garanteix la cobertura i assigna els recursos i els avalua, les entitats proveïdores que ofereixen serveis sanitaris a la població. Es demana l’elaboració d’un codi de governança per a les institucions sanitàries i s’estableixen criteris per la designació d’integrants dels òrgans de govern de les institucions.
Cal dir doncs que aquestes 83 propostes mereixen una lectura detallada. El treball de col·laboració esmerçat ha estat ampli i exemplar. Avui donant resposta al mandat unànime del Parlament de Catalunya, els representants de pacients i usuaris, dels col·legis professionals, d’associacions empresarials, entitats municipalistes, societats científiques, universitats, i grups parlamentaris de CiU i ERC, us presentem aquest document de bases que considerem el fonament per tal que des d’aquest Parlament es faci efectiu un Pacte Nacional de Salut.
Si abans he assenyalat la salut com prioritat humana, el consens de les forces polítiques sobre el sistema de salut esdevé imprescindible. Precisament fa poques setmanes en un article al New England Journal of Medicine, Anne Mills revisava les característiques que tenen els sistemes sanitaris més exitosos: el consens polític n’esdevé una d’elles. I jo diria la primera de totes.
En l’elaboració d’aquest document hi ha una contribució de tots els que han participat a la comissió, també d’entitats i grups polítics que avui no han pogut donar suport a aquestes propostes. He de dir-vos que pertoca a aquesta cambra el poder fer efectiu aquest consens que desitja la ciutadania, les bases perquè això sigui possible hi són només cal teixir-les acuradament i amb generositat.
Permeteu-me que com a coordinador expressi un sentiment compartit, aquest Parlament ens ha donat l’opció de mostrar el sistema sanitari que desitgem i volem agrair-ho. Això no passa cada dia, avui és un moment singular. El país es troba en un moment singular, tots ho sabem. Algunes de les respostes al sistema sanitari que desitgem rauen precisament en una capacitat d’autogovern. És així doncs que la política i la política sanitària han d’anar de bracet. Aquest és el moment de la política en majúscules, aquell on cal deixar de banda aspectes menors i concentrar-nos en allò que ens uneix.
Vull agrair al Govern la confiança dipositada en la meva persona per tal de coordinar aquesta comissió. Vaig acceptar de bon grat i vull dir-vos que n’estic molt satisfet de com hem estat capaços de dur-ho a bon terme. Crec que ha estat exemplar, a l’alçada d’un país modern i avançat. Alhora vull agrair sincerament la col.laboració i suport tècnic que he rebut des del Departament de Salut que això ha estat clau per tal que operativament funcionés.
Als membres de la comissió, dir-vos que ha estat una experiència memorable, que personalment hem trabat nous llaços d’amistat i relació i això fa un país més fort.
És amb un esperit constructiu que sabrem afrontar els reptes de la salut de la ciutadania. Desitjo que des d’aquest Parlament s’encomani d’aquest esperit, i entenc que aquestes paraules són compartides pel conjunt de membres de la comissió, per tant esperem que d’aqui en sorgeixi un proper Pacte Nacional de Salut.
I'm really convinced about the relevance of such consensus. From now on, Parliament will have to achieve a final agreement among the parties. Let's wait for a successful closing.
PS. Afterwards I was interviewed at 8TV.
26 de març 2014
Beware of recreational WGS
Clinical Interpretation and Implications of Whole-Genome Sequencing
If some weeks ago I explained the false advertisement case on nutrigenomics, now from JAMA a new alert appears on whole genome sequencing.
If some weeks ago I explained the false advertisement case on nutrigenomics, now from JAMA a new alert appears on whole genome sequencing.
Depending on sequencing platform, a median of 10% (Illumina Inc; range, 5%-34%) to 19% (Complete Genomics Inc; range, 18%-21%) of genes associated with inherited disease and a median of 9% (Illumina Inc; range, 2%-27%) to 17% (Complete Genomics Inc; range, 17%-19%) of ACMG-reportable genes were not covered at a minimum threshold for genetic variant discoveryAs far as this is the first time that such differences are reported between two alternative sequencers over the same sample, new uncertainties arise on the value of recreational genomics.
25 de març 2014
The roots of new governance
Governance in healthcare institutions
As you know, in this blog I quote canadians in many respects. Their "Board of Directors Governance handbook" is a key document for those who want to understand the role of the board in a hospital. I suggest a quick look.
However, last week there was a closer presentation of a document of interest on governance by Consorci Sanitari i Social. The focus is closely related to the current trend towards converting hybrid organizations into public ones following an accounting criteria ESA-95. Some years ago I explained the big transformation in the ownership due to accounting rules! Incredible, but true.
I have always defended management autonomy and these moves were closely related towards less autonomy and more centralization. Right now, I'm repeating the same: we do need a system that is able to introduce the right governance and management. The issue is not only management autonomy it is also a responsible governance, an issue that in the past has been forgotten many times. The document shows the partial roadmap for such evolution. I would prefer to go beyond that and begin a deep review of current ownerhip and contracting in the public system, to improve efficiency.
As you know, in this blog I quote canadians in many respects. Their "Board of Directors Governance handbook" is a key document for those who want to understand the role of the board in a hospital. I suggest a quick look.
However, last week there was a closer presentation of a document of interest on governance by Consorci Sanitari i Social. The focus is closely related to the current trend towards converting hybrid organizations into public ones following an accounting criteria ESA-95. Some years ago I explained the big transformation in the ownership due to accounting rules! Incredible, but true.
I have always defended management autonomy and these moves were closely related towards less autonomy and more centralization. Right now, I'm repeating the same: we do need a system that is able to introduce the right governance and management. The issue is not only management autonomy it is also a responsible governance, an issue that in the past has been forgotten many times. The document shows the partial roadmap for such evolution. I would prefer to go beyond that and begin a deep review of current ownerhip and contracting in the public system, to improve efficiency.
24 de març 2014
Finding consensus in health policy
One of the key features of successful health systems is to achieve wide consensus at a societal level. Citizens have to share common values on the health system that they want. Some time ago I quoted the article by Anne Mills on this topic.
Today we can confirm that the foundations for such consensus have been built. Although unions and some parties have rejected the current text, there is a wide representation of organizations of the Catalan Council of Health. From now on, the discussion will take place in Parliament.
This is good news. You may have a look at the document here and here. There are many new insights and prescriptions to be developed.
Today we can confirm that the foundations for such consensus have been built. Although unions and some parties have rejected the current text, there is a wide representation of organizations of the Catalan Council of Health. From now on, the discussion will take place in Parliament.
This is good news. You may have a look at the document here and here. There are many new insights and prescriptions to be developed.
20 de març 2014
The seed of efficient genomic sequencing
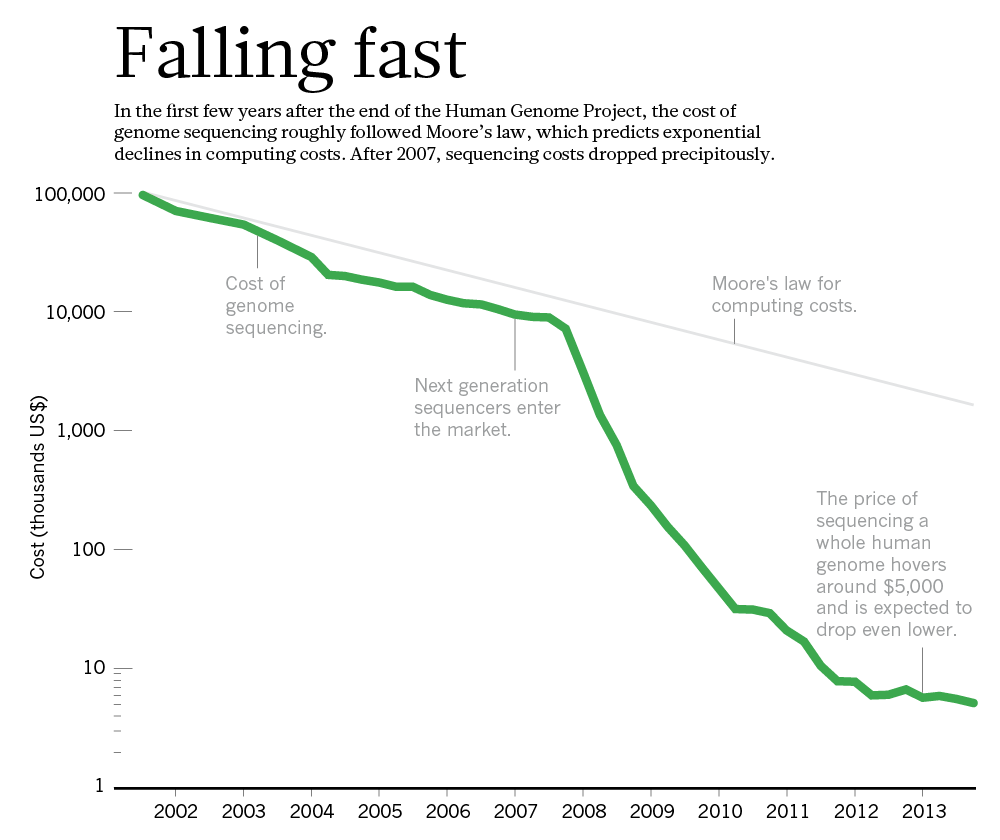
Technology: The $1,000 genome
Imagine for a moment that you have back ten years, and as the health research responsible in the government you decide to allocate $230 million to achieve a $1000 individual genome sequencing. At that moment there was a monopoly by one company, Sanger. Your effort was to promote genomic applied research, better sequencing, and doing so, the monopoly would be undermined.
This is precisely what the US government did through the Advanced sequencing technology awards and right now has achieved its aim, a more efficient sequencing. They have been extremely successful and are closing the program (NHGRI) this year: the goal has been achieved.
The funds allowed to break the former monopoly (Applied Biosystems) and at the same time, ten years later, a new quasi-monopoly has appeared (Illumina). This extraordinary story is well explained in Nature:

Imagine for a moment that you have back ten years, and as the health research responsible in the government you decide to allocate $230 million to achieve a $1000 individual genome sequencing. At that moment there was a monopoly by one company, Sanger. Your effort was to promote genomic applied research, better sequencing, and doing so, the monopoly would be undermined.
This is precisely what the US government did through the Advanced sequencing technology awards and right now has achieved its aim, a more efficient sequencing. They have been extremely successful and are closing the program (NHGRI) this year: the goal has been achieved.
The funds allowed to break the former monopoly (Applied Biosystems) and at the same time, ten years later, a new quasi-monopoly has appeared (Illumina). This extraordinary story is well explained in Nature:
Researchers are optimistic that another technology will emerge to challenge Illumina. Most think, in fact, that the crucial questions for the field will shift away from technology. Now that sequencing is cheap enough to talk about scanning every patient's genome, or at least the protein-coding portion of it, it is still not clear how that information will translate into improved care (see Nature http://doi.org/rvq; 2014). These more complex issues will require another great leap in genomic science — one that could make the trouncing of Moore's law seem easy.
PS. For those that support patents, this is a good example of how prizes substitute patents to spur innovation and confirms Mckinsey article.
19 de març 2014
Medtech on the profitable road
The 2013 Medtech Value Creators Report
Finding Sustainable Value in a Changing Market
Quick numbers from US stock exchange (2009-2013) for 65 companies in Medtech sector (medical device, medical equipment, medical supply and in vitro):
Finding Sustainable Value in a Changing Market
Quick numbers from US stock exchange (2009-2013) for 65 companies in Medtech sector (medical device, medical equipment, medical supply and in vitro):
They generated a TSR (total shareholder return) of 14.8 percent per year. While in terms of value creation its performance trails that of other health-care sectors—such as health care services (at 21.5 percent per year) and biopharmaceuticals (14.9 percent per year)—it has come with less risk (that is, a smaller spread between the TSR values of the best- and the worst-performing companies), thus offering an attractive risk-reward profile for investors.That's all folks.
18 de març 2014
Futility labeling
Choosing Wisely — The Politics and Economics of Labeling Low-Value Services
As far as the evidence on effectiveness is uncertain in some cases, somebody has to put an alert on the population. Asymetric information is always moving towards some bias and favour those with better position. This is the moment for an independent body to disseminate information towards patients. In NEJM you'll find an article about Choosing wisely, an initiative already explained in this blog. An interesting objective, although the means could be controversial. Maybe professional associations are not in best position to assume such task. Kassirer (once again) reflected many years ago the relationships with industry and their conflicts of interest. My suggestion would be independent agencies, NICE style. They should inform population about what works, and they are already doing it.
As far as the evidence on effectiveness is uncertain in some cases, somebody has to put an alert on the population. Asymetric information is always moving towards some bias and favour those with better position. This is the moment for an independent body to disseminate information towards patients. In NEJM you'll find an article about Choosing wisely, an initiative already explained in this blog. An interesting objective, although the means could be controversial. Maybe professional associations are not in best position to assume such task. Kassirer (once again) reflected many years ago the relationships with industry and their conflicts of interest. My suggestion would be independent agencies, NICE style. They should inform population about what works, and they are already doing it.
16 de març 2014
Keep on improving
On the improvement of blood sample collection at clinical laboratories
Efficiency in healthcare management comes as the result of many decisions and actions. Knowledge can improve such decisions. This weekend I was reading this article on clinical labs and how to collect samples with less routes. With operations research techniques, it is possible. Afterwards there is a need to implement them. The results of the article:
Efficiency in healthcare management comes as the result of many decisions and actions. Knowledge can improve such decisions. This weekend I was reading this article on clinical labs and how to collect samples with less routes. With operations research techniques, it is possible. Afterwards there is a need to implement them. The results of the article:
The two laboratories in this study previously planned routes manually for 43 and 74 collection points, respectively. These routes were covered by an external carrier company. With the implementation of this algorithm, the number of routes could be reduced from ten to seven in one laboratory and from twelve to nine in the other, which represents significant annual savings in transportation costsThe potential for operations research in healthcare is huge. The incentives to apply it, low (unfortunately).
13 de març 2014
Commercialism in health and medicine
Buying Health: The Costs of Commercialism and an Alternative Philosophy
There are only three topics of health policy in the newspapers (unfortunately): waiting lists, copayments and privatization. As soon as one topic drops from the agenda, the informational cascade starts with the following one. The last one, privatization is still a concept in need of definition and measurement. I already covered this issue last year and I don't want to repeat it.
Today I would like to insist that beyond a new framing of the concept, maybe we have to change the scope and the term. The right term could be commercialism. We have to understand better how and when commercialism is undermining professionalism.
Jerome Kassirer wrote an excellent piece (US oriented) in Cambridge Quarterly of Healthcare Ethics some years ago that it is still a reference for today. His words:
Churchill and Churchill go beyond the usual scope. Their recent article abstract says:
There are only three topics of health policy in the newspapers (unfortunately): waiting lists, copayments and privatization. As soon as one topic drops from the agenda, the informational cascade starts with the following one. The last one, privatization is still a concept in need of definition and measurement. I already covered this issue last year and I don't want to repeat it.
Today I would like to insist that beyond a new framing of the concept, maybe we have to change the scope and the term. The right term could be commercialism. We have to understand better how and when commercialism is undermining professionalism.
Jerome Kassirer wrote an excellent piece (US oriented) in Cambridge Quarterly of Healthcare Ethics some years ago that it is still a reference for today. His words:
Professionalism is fundamentally a pact with society. In recognition of certain behaviors and attributes, society confers professional status on us. These privileges are not bestowed, but are earned, and they must be renewed repeatedly for the status to be preserved. Professional behaviors include technical competence that is valued and that adds value, a commitment to self-improvement, a commitment to selfmonitoring and self regulation, and a commitment to use the unique knowledge and competence for the best interests of our patients. This last requirement should include a commitment to resolve conflicts of interest in our patients’ favor.
Is money trumping professionalism? Certainly the pharmaceutical money tsunami is having major adverse effects. It tends to distract faculty into emphasizing profitable research and to neglect their teaching duties. It replaces openness with secrecy, it privatizes knowledge, and it replaces part of the social commons by commercializing discovery. In many instances, it downplays knowledge as a social good. It has also created a culture within which the design of studies is sometimes jiggered to create positive results, in which unfavorable results are sometimes buried, where communication of results is sometimes hindered for commercial reasons, and where bias in publications and educational materials has gone completely uncheckedMaybe there are excessive generalizations, but take it as a general statement to be confirmed by facts and data.
Churchill and Churchill go beyond the usual scope. Their recent article abstract says:
This paper argues that commercial forces have steadily encroached into our understanding of medicine and health in modern industrial societies. The impact on the delivery of personal medical services and on common ideas about food and nutrition is profound and largely deleterious to public health. A key component of commercialization is reductionism of medical services, health products and nutritional components into small, marketable units. This reductive force makes both medical services and nutritional components more costly and is corrosive to more holistic concepts of health. We compare commercial and holistic approaches to nutrition in detail and offer an alternative philosophy. Adopting this alternative will require sound public policies that rely less on marketing as a distribution system and that enfranchise individuals to be reflective on their use of medical services, their food and nutrition choices, and their larger health needsI deeply agree with such perspective.
12 de març 2014
Against patents, again
Deadly Monopolies: The Shocking Corporate Takeover Of Life Itself – And The Consequences For Your Health And Our Medical Future
I've just finished reading a book on patents in life sciences. As you know from previous posts , I'm convinced that there is an enormous welfare loss from current patent system. If you have the opportunity to read this book, you'll finally will arrive at the same conclusion. Although it was written before the Supreme Court ruling over the Myriad case, the message is still the same: patents contrain innovation and are extremely costly to the society. The case of Hepatitis C is explained in detail. Until some patents were exhausted there was no possibility to start research. Without such patents, new succesful and (costly) treatments have arisen (and afterwards have been patented again).
An interesting interview in Forbes magazine highlights the key issues of the book. Unfortunately times go by and alternatives to patents are not taking off.
I've just finished reading a book on patents in life sciences. As you know from previous posts , I'm convinced that there is an enormous welfare loss from current patent system. If you have the opportunity to read this book, you'll finally will arrive at the same conclusion. Although it was written before the Supreme Court ruling over the Myriad case, the message is still the same: patents contrain innovation and are extremely costly to the society. The case of Hepatitis C is explained in detail. Until some patents were exhausted there was no possibility to start research. Without such patents, new succesful and (costly) treatments have arisen (and afterwards have been patented again).
An interesting interview in Forbes magazine highlights the key issues of the book. Unfortunately times go by and alternatives to patents are not taking off.
10 de març 2014
Health impact of sugar-sweetened beverages taxation
Averting Obesity and Type 2 Diabetes in India through Sugar-Sweetened Beverage Taxation: An Economic-Epidemiologic Modeling Study
Clever politicians want to know the potential welfare impact of taxation. I said "clever", though this is not always the case. An example of economic modeling for sugar-sweetened beverages to set up the right level of taxation (in India), appears in PLOS Medicine. The summary:
The documentary is about weight control, but places special emphasis on sugar (addiction). Please have a look at the quantity of sugar in a beverage!!! (14 sugar cubes). Incredible.
PS. "Superbe" post by Reinhardt: How the Medical Establishment Got the Treasury’s Keys
Clever politicians want to know the potential welfare impact of taxation. I said "clever", though this is not always the case. An example of economic modeling for sugar-sweetened beverages to set up the right level of taxation (in India), appears in PLOS Medicine. The summary:
The researchers used survey data relating SSB consumption to price variations to calculate how changes in the price of SSBs affect the demand for SSBs (own-price elasticity) and for other beverages (cross-price elasticity) in India. They combined these elasticities and data on SSB sales trends, BMIs, and diabetes incidence (the frequency of new diabetes cases) into a mathematical microsimulation model to estimate the effect of a 20% tax on SSBs on caloric (energy) consumption, glycemic load (an estimate of how much a food or drink raises blood sugar levels after consumption; low glycemic load diets lower diabetes risk), the prevalence of overweight/obesity, and the incidence of diabetes among Indian subpopulations. According to the model, if SSB sales continue to increase at the current rate, compared to no tax, a 20% SSB tax would reduce overweight/obesity across India by 3.0% and the incidence of type 2 diabetes by 1.6% over the period 2014–2023. In absolute figures, a 20% SSB tax would avert 11.2 million cases of overweight/obesity and 400,000 cases of type 2 diabetes between 2014 and 2023. Notably, if SSB sales increase more steeply as predicted by drinks industry marketing models, the tax would avert 15.8 million cases of overweight/obesity and 600,000 cases of diabetes. Finally, the model predicted that the largest relative effect of an SSB tax would be among young men in rural areas.The results confirm previous studies, 20% may be the ceiling for a tax . But what happens to health?. Assumptions on a fall in consumption, are just that, assumptions. And former behaviour is extrapolated into the future. This is what happens to any model, and this is the uncertainty and courage that any politician must hold in taking a difficult decision. Such moment is closer than before. If you are not convinced, I would suggest you have a look at this documentary released last week:
The documentary is about weight control, but places special emphasis on sugar (addiction). Please have a look at the quantity of sugar in a beverage!!! (14 sugar cubes). Incredible.
PS. "Superbe" post by Reinhardt: How the Medical Establishment Got the Treasury’s Keys
07 de març 2014
Cost-effectiveness with uncertain effectiveness
Gene expression testing is quite different from genetic testing. Gene expression refers to epigenetic regulation of genes that occur without alteration of DNA. I've covered such topics several times in this blog. Today, I would like to focus on a recent published work on a new test that assesses whether or not a patient's chest discomfort or other symptoms are due to obstructive coronary artery disease. Sounds interesting, since angiography is a costly technology.
A quick look at this recent article will raise new doubts. As you know, there is no need for cost-effectiveness analysis when effectiveness is uncertain. When talking about testing effectiveness means, sensitivity and specificity, AUC and so on. But what happens when the seller (or the model) decides about the threshold and afterwards focuses on negative predictive value of 96% and provides the desired value?. The threshold is only an option in the model. Why not change it?. There is a circular reasoning on that.
My concern is that health economics should look in detail at such issues. It is not an issue of conflicts of interest. In this case any health economist should avoid entering such territory.
05 de març 2014
When asking your physician is not enough
23andMe and the FDA
Some weeks ago I explained the FDA "closure" of DTC genetic testing business. NEJM analyses with detail the rationale behind such policy:
Some weeks ago I explained the FDA "closure" of DTC genetic testing business. NEJM analyses with detail the rationale behind such policy:
The goal of the FDA and 23andMe (as well as all clinical geneticists, testing laboratories, and the entire genetics industry) should be to ensure that genomic information is both accurate and clinically useful. Clinicians will be central to helping consumer–patients use genomic information to make health decisions. Any regulatory regime must recognize this reality by doing more than simply adding the tagline on most consumer ads for prescription drugs: “Ask your physician.” That is insufficient guidance unless your physician has ready access to a clinical geneticist or genetic counselor.European regulation is 15 years old and the new directive is still being discussed. It will not be applied for at least 3 years. Meanwhile, do you know who is protecting us from inaccurate and clinically useless information?
04 de març 2014
Let's get fit, not fat
Aportaciones de la economía del comportamiento en política sanitaria: Algunas notas en torno al ejemplo de la obesidad
The influence of obesity and overweight on medical costs: a panel data perspective
In the EJHE you'll find a clear message:
The EEA article by A. Garcia-Altés reflects current knowledge on behavioral economics and obesity. However there is a long way to go. As I said in a former post we do need a battery of measures to fight obesity: regulatory, social and individual measures.
The influence of obesity and overweight on medical costs: a panel data perspective
In the EJHE you'll find a clear message:
The results indicate that obesity is associated with substantial healthcare cost increases and there are large differences in costs by degree of obesity. Specifically, severe obesity raises total direct medical costs by an average of 160 € per patient and year. With total medical costs averaging 600 € for normal-weight individuals, this means that severe obesity is associated with an increase in costs of 26 %. The effect of moderate obesity is more modest: it raises medical costs by 97 € or 16 %. Overweight has an even smaller impact, raising costs by 51 € or 8.5 %.Therefore, if obesity has an economic and health impact, what next?
The EEA article by A. Garcia-Altés reflects current knowledge on behavioral economics and obesity. However there is a long way to go. As I said in a former post we do need a battery of measures to fight obesity: regulatory, social and individual measures.
28 de febrer 2014
Our irrational behaviour
The Behavioral Economics of Health and Health Care
Irrationality in Health Care: What Behavioral Economics Reveals About What We Do and Why
Thomas Rice provides an overview of behavioral economics in health in a recent article in Annual review of public health. More or less the same things we already know with some concrete messages. A good starting point for those that want to take first steps in this discipline. The summary:
Thomas Rice says in this respect:
PS. For those interested in an introductory course, on March 11th starts at Coursera: A Beginner's Guide to Irrational Behavior
Irrationality in Health Care: What Behavioral Economics Reveals About What We Do and Why
Thomas Rice provides an overview of behavioral economics in health in a recent article in Annual review of public health. More or less the same things we already know with some concrete messages. A good starting point for those that want to take first steps in this discipline. The summary:
People often make decisions in health care that are not in their best interest, ranging from failing to enroll in health insurance to which they are entitled, to engaging in extremely harmful behaviors. Traditional economic theory provides a limited tool kit for improving behavior because it assumes that people make decisions in a rational way, have the mental capacity to deal with huge amounts of information and choice, and have tastes endemic to them and not open to manipulation. Melding economics with psychology, behavioral economics acknowledges that people often do not act rationally in the economic sense. It therefore offers a potentially richer set of tools than provided by traditional economic theory to understand and influence behaviorsRight now behavioral economics is still a promise, let's wait until we can really apply it widely.
Thomas Rice says in this respect:
With the exception of Kahneman & Tversky’s prospect theory, which was developed more than 30 years ago, there has been little in the way of bringing the various tools and policies of behavioral economics under one umbrella. As a result, most of the applications seem to be ad hoc. More development of an overarching theory could aid those interested in designing new interventions when it is clear that traditional economics remedies are insufficientRegarding the book on Irrationality in Health Care, I haven't had the opportunity to have a look at it. I leave here the reference and 23 anomalies . Maybe in the book there is the answer to solve them.
PS. For those interested in an introductory course, on March 11th starts at Coursera: A Beginner's Guide to Irrational Behavior
27 de febrer 2014
Hostis populi
A plot written by Ibsen in 1882 could reflect current conflicts nowadays. Whats first: Your money or your health?. I went to the theatre last week. Great "mise en escène".
The summary:
The summary:
Doctor Thomas Stockmann is a popular citizen of a small coastal town in Norway. The town has invested a large amount of public and private money towards the development of baths, a project led by Stockmann and his brother, Peter, the Mayor. The town is expecting a surge in tourism and prosperity from the new baths, which are said to be of great medicinal value, and as such, a source of great local pride. Just as the baths are proving successful, Stockmann discovers that waste products from the town's tannery are contaminating the waters, causing serious illness amongst the tourists. He expects this important discovery to be his greatest achievement, and promptly sends a detailed report to the Mayor, which includes a proposed solution which would come at a considerable cost to the town.I deeply disagree with this final generalization. The details are important.
To his surprise, Stockmann finds it difficult to get through to the authorities. They seem unable to appreciate the seriousness of the issue and unwilling to publicly acknowledge and address the problem because it could mean financial ruin for the town. As the conflict develops, the Mayor warns his brother that he should "acquiesce in subordinating himself to the community." Stockmann refuses to accept this, and holds a town meeting at Captain Horster's house in order to persuade people that the baths must be closed.
The townspeople — eagerly anticipating the prosperity that the baths will bring — refuse to accept Stockmann's claims, and his friends and allies, who had explicitly given support for his campaign, turn against him en masse. He is taunted and denounced as a lunatic, an "Enemy of the People." In a scathing rebuttal of both the Victorian notion of community and the principles of democracy, Stockmann proclaims that, in matters of right and wrong, the individual is superior to the multitude, which is easily led by self-advancing demagogues. Stockmann sums up Ibsen's denunciation of the masses with the memorable quote "...the strongest man in the world is the man who stands most alone." He also says: "A minority may be right; a majority is always wrong.
26 de febrer 2014

The quality cure into action
The next David Cutler book: "The Quality Cure. How Focusing on Health Care Quality Can Save Your Life and Lower Spending Too" will appear in April. Meanwhile we can read some pages from Google Books. He sets "quality" at the top of the agenda and he explains that Obamacare is trying to solve access. Focusing on quality means effort on greater value, avoiding waste, and therefore cost containment. At the begining it may seem an already heard message, however I agree with him that the quality chasm must be addressed, as well in our country. The book is a must read beyond US borders for any person involved in health care as it is his former book "Your money or your life" . The first statements from the preface:
PS. A former post on this blog about David Cutler.
PS. On conflicts of interest in medicine. The paper on "The burden of disclosure" by Loewenstein et al. And the comment by Alex Fradera.
For decades, health care was like the weather-everybody talked about it, but nobody did anything about it. Talk was easy, politicians and analysts of all stripe agreed that we wanted a health care system focused on preventing disease and treating it appropriately when necessary. In the past half decade, talk has turned into action.Let's apply his final words, it's time to turn talk into action.
PS. A former post on this blog about David Cutler.
PS. On conflicts of interest in medicine. The paper on "The burden of disclosure" by Loewenstein et al. And the comment by Alex Fradera.
25 de febrer 2014
The hole for genetic testing market entry
Technology Assessment on Genetic Testing or Molecular Pathology Testing of Cancers with Unknown Primary Site to Determine Origin
Update on Emerging Genetic Tests Currently Available for Clinical Use in Common Cancers
AHRQ has just published two reports of interest. The first is devoted to assess the evidence on the analytical validity, clinical validity, and clinical utility of commercially available genetic tests for identifying the tissue of origin (TOO) of the cancer in patients with cancer of unknown primary (CUP) site. The second describes genetic tests that have applications in the common solid tumors (breast, lung, colorectal, pancreas, etc.) as well as tests that are used in hematologic cancers (leukemia, lymphoma) and are already available in clinical practice.While the first is an assessment, the second is informative.
There is still a third report to be released and meanwhile NRD explains its conclusions. Having selected 11 prognostic tests, only around half had evidence supporting their prognostic accuracy or clinical validity. Therefore the question is always the same: why these tests without evidence are on the market? Why have they been approved by the FDA?. There is a big regulatory hole to fill in.
Update on Emerging Genetic Tests Currently Available for Clinical Use in Common Cancers
AHRQ has just published two reports of interest. The first is devoted to assess the evidence on the analytical validity, clinical validity, and clinical utility of commercially available genetic tests for identifying the tissue of origin (TOO) of the cancer in patients with cancer of unknown primary (CUP) site. The second describes genetic tests that have applications in the common solid tumors (breast, lung, colorectal, pancreas, etc.) as well as tests that are used in hematologic cancers (leukemia, lymphoma) and are already available in clinical practice.While the first is an assessment, the second is informative.
There is still a third report to be released and meanwhile NRD explains its conclusions. Having selected 11 prognostic tests, only around half had evidence supporting their prognostic accuracy or clinical validity. Therefore the question is always the same: why these tests without evidence are on the market? Why have they been approved by the FDA?. There is a big regulatory hole to fill in.
24 de febrer 2014
Conflicts of interest (in medicine)
I would like to attend this seminar:
Professor George Lowenstein
Behavioural Economics and Conflicts of Interest
Lecture Theatre 3, Cambridge Judge Business School. Tuesday 25th February 5-6.30pm. No need to register but arrive early in order to get a seat.
Unfortunately, I can't attend. Any info will be appreciated.
You may follow events on Behavioral Economics, here.
PS. Our public expenditure on health on 2012 gave ground, and was close to 5 years before: 2007. Such expenditure over GDP is still at 2008 position: 5,3% , while our GDP per capita (27.442€) is at levels before 2006 (!). Therefore we are spending on health (more than) proportionally to our GDP historical trend, however our GDP has shrinked a lot. And we maintain distance to OECD average health expenditure (6,69%) although our per capita GDP is 2,7% larger. That's all right now, it's an issue of months.
PS. Interesting post by Josep Maria Via.
Professor George Lowenstein
Behavioural Economics and Conflicts of Interest
“A conflict of interest is a clash between an individual’s professional responsibilities and their personal, typically financial, interests. Traditional economics has not shed much light on conflicts of interest, perhaps in part because it has not recognized the importance of professionalism as a motive in human behaviour. In this talk I will present results from a variety of studies that examine the behavioural economics of conflict of interest. Focusing mainly on conflicts of interest in medicine, some of the research shows how people who care deeply about behaving in a professional fashion can be corrupted by economic incentives. Other research shows how disclosing conflicts of interest, far from helping the recipient of information, can backfire, helping the advice-giver and hurting the advice recipient.”
Lecture Theatre 3, Cambridge Judge Business School. Tuesday 25th February 5-6.30pm. No need to register but arrive early in order to get a seat.
Unfortunately, I can't attend. Any info will be appreciated.
You may follow events on Behavioral Economics, here.
PS. Our public expenditure on health on 2012 gave ground, and was close to 5 years before: 2007. Such expenditure over GDP is still at 2008 position: 5,3% , while our GDP per capita (27.442€) is at levels before 2006 (!). Therefore we are spending on health (more than) proportionally to our GDP historical trend, however our GDP has shrinked a lot. And we maintain distance to OECD average health expenditure (6,69%) although our per capita GDP is 2,7% larger. That's all right now, it's an issue of months.
PS. Interesting post by Josep Maria Via.
20 de febrer 2014
The market size of stratified medicine
Defining and quantifying the use of personalized medicines
There is a lot of noise around the message that the personalised-stratified medicine era has arrived. If you split the clamour from the message, the result is close to 34 medicines at the end of 2012, and in market volume accounted for 3% of the global market by the end of 2009. You'll find this details at NRD and this is the key comment:
There is a lot of noise around the message that the personalised-stratified medicine era has arrived. If you split the clamour from the message, the result is close to 34 medicines at the end of 2012, and in market volume accounted for 3% of the global market by the end of 2009. You'll find this details at NRD and this is the key comment:
First, in terms of characteristics, oncology agents dominate personalized medicine utilization, and disproportionately address unmet medical needs as revealed by priority, accelerated, and orphan disease FDA designations. Second, older drugs that have become personalized medicines post-launch have had a significant impact on the growth of small-molecule personalized medicines; however, the translation from label to clinical practice remains uncertain. Third, per capita usage of personalized medicines in the EU5 markets is greater than in the United States, with usage rates in Japan and the rest of the world growing rapidly
Affair in Cascais
Club des Belugas- the Chin Chin Sessions
19 de febrer 2014
Everything is connected
Pla Interdepartamental de Salut Pública
We all know that improving population health is a task that exceeds the healthcare system. The political debate is too focused on healthcare rather than other determinants to improve health. However, today is a different day. A new plan to introduce health in all policies has been approved and this means a change in the agenda. We'll see how this will be managed, since it is a new approach.
Have a look at the document. The authors have been working hard for months on it. Such policy follows EU criteria and represents an innovation in the current health policy landscape. Let's see how effective it is.
We all know that improving population health is a task that exceeds the healthcare system. The political debate is too focused on healthcare rather than other determinants to improve health. However, today is a different day. A new plan to introduce health in all policies has been approved and this means a change in the agenda. We'll see how this will be managed, since it is a new approach.
Have a look at the document. The authors have been working hard for months on it. Such policy follows EU criteria and represents an innovation in the current health policy landscape. Let's see how effective it is.
18 de febrer 2014
Capitalism and morality
Market Reasoning as Moral Reasoning: Why Economists Should Re-engage with Political Philosophy
I found this article. Have a look at the abstract:
I found this article. Have a look at the abstract:
In my book What Money Can't Buy: The Moral Limits of Markets (2012), I try to show that market values and market reasoning increasingly reach into spheres of life previously governed by nonmarket norms. I argue that this tendency is troubling; putting a price on every human activity erodes certain moral and civic goods worth caring about. We therefore need a public debate about where markets serve the public good and where they don't belong. In this article, I would like to develop a related theme: When it comes to deciding whether these or those goods should be allocated by the market or by nonmarket principles, economics is a poor guide. Deciding which social practices should be governed by market mechanisms requires a form of economic reasoning that is bound up with moral reasoning. But mainstream economic thinking currently asserts its independence from the contested terrain of moral and political philosophy. If economics is to help us decide where markets serve the public good and where they don't belong, it should relinquish the claim to be a value-neutral science and reconnect with its origins in moral and political philosophy.There are health economics implications, with a little effort you can find them.
17 de febrer 2014
Effectiveness, first things first
Homeopathy in Healthcare – Effectiveness, Appropriateness,Safety, CostsAn HTA report on homeopathy as part of the Swiss Complementary Medicine Evaluation Programme
Swiss government requested a report on homeopathy through the Complementary Medicine Evaluation Program, just to understand its cost-effectiveness. You'll find the complete story in this blog.
The key table is here.Such report and this table created controversy due to conflicts of interest of their authors.
Finally the government decided not to include homeopathy in the reimbursed benefit basket.
Is there any reason to regulate when the effectiveness has not been demonstrated?. This is my question today to a regulator that it seems busy on this issue. My answer is clear, it is unnecessary. He has to inform the citizens and incriminate providers in case of false advertising.
PS. I already said this before, here and here .
Swiss government requested a report on homeopathy through the Complementary Medicine Evaluation Program, just to understand its cost-effectiveness. You'll find the complete story in this blog.
The key table is here.Such report and this table created controversy due to conflicts of interest of their authors.
Finally the government decided not to include homeopathy in the reimbursed benefit basket.
Is there any reason to regulate when the effectiveness has not been demonstrated?. This is my question today to a regulator that it seems busy on this issue. My answer is clear, it is unnecessary. He has to inform the citizens and incriminate providers in case of false advertising.
PS. I already said this before, here and here .
13 de febrer 2014
Competing on biosimilars
One year ago McKinsey released a report on biosimilars. They explained what happened in Europe after 2005 regulation. Now NRD has published an interesting article by Henry Grabowsky et al. that shows wide differences within Europe. In Germany, 42% of the market of Epoetin is biosimilar, while UK remains at 7,9% (!). The article explains the reasons behind such variation. If we have to summarise in one cause, this would be: incentive regulation. And since prices are 25% less than original products, such difference has high opportunity costs for UK citizens (however the price levels in Germany is higher than the UK).
In their words:
PS. IMS presentation.
In their words:
One major finding is that the competitive performance of the biosimilars we analysed in Europe is mixed both across countries and products. Although the European Union has a common regulatory system for approving biosimilars, differences in reimbursement practices and incentives as well as variations in medical practices have resulted in different outcomes across countries.Does anybody know what's happening here?
PS. IMS presentation.
12 de febrer 2014
What is the rule of law?
If we look around us these days we can detect that these conditions have mostly vanished in many public environments:
There is one and only option: disconnect asap and forget this nightmare.
PS. I said something similar one year and a half ago.
PS. Is there any price-cap on publicly funded drugs? In France, the recommendation is to limit any new drug to 50.000€. You'll find it here p.15. Let's see what really happens here. In UK, confidential discounts apply. Welcome to the transparent world!. Have a look at my previous post on the same topic and the table.
PS. Lewis Mumford dixit:
"For most Americans, progress means accepting what is new because it is new, and discarding what is old because it is old. This may be good for a rapid turnover in business, but it is bad for continuity and stability in life. Progress, in an organic sense, should be cumulative, and though a certain amount of rubbish-clearing is always necessary, we lose part of the gain offered by a new invention if we automatically discard all the still valuable inventions that preceded it.”
- The government and its officials and agents as well as individuals and private entities are accountable under the law.
- The laws are clear, publicized, stable and just, are applied evenly, and protect fundamental rights, including the security of persons and property.
- The process by which the laws are enacted, administered and enforced is accessible, fair and efficient.
- Justice is delivered timely by competent, ethical, and independent representatives and neutrals who are of sufficient number, have adequate resources, and reflect the makeup of the communities they serve.
- Social and therapeutic value of the drug and incremental clinical benefit, taking into account its cost-effectiveness relationshipNew drugs are being accepted every month, and since June 2012 the Health Ministry hasn't updated the website. Nobody knows its cost-effectiveness. Some weeks ago a transparency law was approved. It's a joke.
There is one and only option: disconnect asap and forget this nightmare.
PS. I said something similar one year and a half ago.
PS. Is there any price-cap on publicly funded drugs? In France, the recommendation is to limit any new drug to 50.000€. You'll find it here p.15. Let's see what really happens here. In UK, confidential discounts apply. Welcome to the transparent world!. Have a look at my previous post on the same topic and the table.
PS. Lewis Mumford dixit:
"For most Americans, progress means accepting what is new because it is new, and discarding what is old because it is old. This may be good for a rapid turnover in business, but it is bad for continuity and stability in life. Progress, in an organic sense, should be cumulative, and though a certain amount of rubbish-clearing is always necessary, we lose part of the gain offered by a new invention if we automatically discard all the still valuable inventions that preceded it.”
11 de febrer 2014
A disruptive global health policy agenda
The political origins of health inequity: prospects for change
In order to understand the roots of health inequality, political and institutional factors are crucial. However, they are difficult to assess and identify. This is precisely what Lancet does with the new initiative on Global Governance for Health. As you may know, I'm not a fan of certain approaches and research on inequality, however this document is a milestone to understand where we are and where global health policy should go. Just a caveat, somebody may consider that it is naïf to call for global governance for health if we are not able to define a global governance for peace (e.g. Siria). I'm among those.
PS. After reading this article at EP I'm convinced that we need to define governance mechanisms for better public management. The devil is in the details.
PS. A failed state is voting today against universal justice to avoid prosecution of Tibet genocide responsible. What a shame!, those that are voting the proposal should have been in a tibetan skin and they would change their minds.
PS. The Day We Fight Back against mass surveillance
In order to understand the roots of health inequality, political and institutional factors are crucial. However, they are difficult to assess and identify. This is precisely what Lancet does with the new initiative on Global Governance for Health. As you may know, I'm not a fan of certain approaches and research on inequality, however this document is a milestone to understand where we are and where global health policy should go. Just a caveat, somebody may consider that it is naïf to call for global governance for health if we are not able to define a global governance for peace (e.g. Siria). I'm among those.
PS. After reading this article at EP I'm convinced that we need to define governance mechanisms for better public management. The devil is in the details.
PS. A failed state is voting today against universal justice to avoid prosecution of Tibet genocide responsible. What a shame!, those that are voting the proposal should have been in a tibetan skin and they would change their minds.
PS. The Day We Fight Back against mass surveillance
Club des Belugas. Trip to Saint Topez from Chin Chin Sessions album.
Great Music
10 de febrer 2014
Time to refocus
Better health, better care, better value for all
Canada Health Council has analysed the impact of health reform one decade later. The report is worth reading, as long as it is full of details of what worked and what didn't. Despite the commitment to primary care, things didn't change as expected. They have to refocus. A key paragraph:
PS. Avoiding waste, Value-based medicine at GCVarela
Canada Health Council has analysed the impact of health reform one decade later. The report is worth reading, as long as it is full of details of what worked and what didn't. Despite the commitment to primary care, things didn't change as expected. They have to refocus. A key paragraph:
Governments think only in terms of office, citizens perspective focus on long-term welfare. Fortunately for Canadians, the council cares for a long-term performance assessment of health policies.Although the resources to improve our health system and the health of Canadians were made available, the success of the health accords in stimulating health system reform was limited. Overall, the decade saw few notable improvements on measures of patient care and health outcomes, and Canada’s performance compared to other high-income countries is disappointing. Some pressing issues have been addressed including wait times, primary health care reform, drug coverage, and physicians’ use of electronic health records. But none of these changes have transformed Canada’s health system into a high-performing one, and health disparities and inequities continue to persist across the country.
PS. Avoiding waste, Value-based medicine at GCVarela
06 de febrer 2014
Context and evidence based health policy
Health Care Systems in Low- and Middle-Income Countries
What works?. This is a difficult question. And this is exactly the issue that Anne Mills is addressing in her NEJM article. Her review of health systems in low and middle-income countries achieves and inconvenient but true conclusion:
I believe that such characteristics hold as well for high-income countries. Evidence for health policy is context based. No universal laws for implementation, only some criteria, some characteristics. Food for thought.
PS. " Our research suggests that the economics of vertical integration makes sense for payors in only a minority of markets.". McKinsey guys at HA blog. I agree.
What works?. This is a difficult question. And this is exactly the issue that Anne Mills is addressing in her NEJM article. Her review of health systems in low and middle-income countries achieves and inconvenient but true conclusion:
On the basis of the evidence presented above, few clear-cut conclusions can be drawn with regard to the best strategies for strengthening countries' health care systems. An approach that works well in one country may work less well in another, and not all approaches are equally acceptable to all governments or their multiple constituencies. There is no one blueprint for an ideal health care system, nor are there any magic bullets that will automatically elicit improved performance. This is hardly surprising: health care systems are complex social systems,31 and the success of any one approach will depend on the system into which it is intended to fit as well as on its consistency with local values and ideologies.
A recent historical study of the contribution of the health care system to improved health in five countries identified a number of characteristics of successful health care systems Such systems were able to develop the capacity to select promising strategies and to learn from the efforts of other countries as well as from their own experimentation. The strengthening of a health care system requires a focus not only on specific strategies, such as those considered above, but also on the creation of an environment that supports innovation. Health care strengthening must thus be seen as a long-term process that involves complex systems and requires carefully orchestrated action on a number of fronts. The global community can help by supporting country-led processes of reform and by helping to create a stronger evidence base that contributes to cross-country learning.
I believe that such characteristics hold as well for high-income countries. Evidence for health policy is context based. No universal laws for implementation, only some criteria, some characteristics. Food for thought.
PS. " Our research suggests that the economics of vertical integration makes sense for payors in only a minority of markets.". McKinsey guys at HA blog. I agree.
05 de febrer 2014
False advertising
The concern over consumer protection is growing with new health technologies. This is not new, you may think. However the lawsuit by FTC against Genelink for misleading claims is the first case in a genetics testing company. Genelink said that they analyzed your DNA and afterwards send back nutritional supplements customized to your personal genome. The regimen, the company promised, was good for diabetes, heart disease, arthritis, insomnia and other ailments.On request by FTC, they were unable to confirm such promises.
Since you may find a similar test on the corner of the street, once again my question is: where is the regulator?
PS. Some months ago, was the FDA who asked 23and me to stop selling its genetics test kit.
PS. On DTC genetic tests, a good article.
Since you may find a similar test on the corner of the street, once again my question is: where is the regulator?
PS. Some months ago, was the FDA who asked 23and me to stop selling its genetics test kit.
PS. On DTC genetic tests, a good article.
31 de gener 2014
An ongoing tug-of-war
Understanding Differences Between High- And Low-Price Hospitals: Implications For Efforts To Rein In Costs
Consolidation of private healthcare providers is an increasing trend nowadays. The exact implications for competition and choice are usually unknown. It is worth having a look at other markets. This article in HA explains the impact for the US context:
PS. On limiting bisphenol in food.
PS. Health expenditures NEJM Graphic
PS.Health Policy Basics: Health Insurance Marketplaces
PS. Are Human Genes Patentable?
PS. Regulating 23andMe to Death Won’t Stop the New Age of Genetic Testing
Consolidation of private healthcare providers is an increasing trend nowadays. The exact implications for competition and choice are usually unknown. It is worth having a look at other markets. This article in HA explains the impact for the US context:
PS. HA Blog, a comment.Prior research shows that private hospital prices vary considerably both within and across markets, even after differences in patient populations and services provided are accounted for. The wide variations in price and the high prices at some hospitals reflect an ongoing tug-of-war between increasingly consolidated buyers (health plans) and increasingly consolidated sellers (hospitals and hospital systems).Given the intense and growing pressure to rein in the growth in private health insurance premiums, the continuation of current trends appears to be unsustainable. It remains to be seen whether or not health plans will somehow regain the upper hand. If they do not, more radical approaches—such as state-based rate setting or restrictions on contracting arrangements between hospitals and health plans—may gain traction.
PS. On limiting bisphenol in food.
PS. Health expenditures NEJM Graphic
PS.Health Policy Basics: Health Insurance Marketplaces
PS. Are Human Genes Patentable?
PS. Regulating 23andMe to Death Won’t Stop the New Age of Genetic Testing
29 de gener 2014
Who is the owner?
While reading a recent op-ed on hospitals in a National Health System, suddenly I asked myself: but who is the owner?. The article was reflecting a new view on hierarchy and management of public organizations and was advocating for new cooperative models, horizontal schemes where professionals fit better than a pure civil servant. It may sound good, although it raises a certain fuzzy landscape. Who has the decision rights in a cooperative scheme? Who is the residual claimant?. Just check The Economist for a recent case and remember the potential implications if we translate such model in health care.
There are two sides of the coin: management and governance. Managers and owners have their specific roles. When somebody wants to play both, conflicts of interest arise. It's obvious. Unfortunately in public organizations, such considerations are too often forgotten. Public organizations require better governance designs, stronger and clearer, representing the preferences of the final owner: the citizen.
There are two sides of the coin: management and governance. Managers and owners have their specific roles. When somebody wants to play both, conflicts of interest arise. It's obvious. Unfortunately in public organizations, such considerations are too often forgotten. Public organizations require better governance designs, stronger and clearer, representing the preferences of the final owner: the citizen.
27 de gener 2014
TMT syndrome
What It Will Take To Achieve The As-Yet-Unfulfilled Promises Of Health Information Technology?
Each day every newspaper wants to convince us over a new technology. In biosciences, journalists enjoy talking about "opening doors" to new cures, and rarely anybody checks afterwards if this anouncement is really in place and provides its expected outcomes. Most of what we see in the media regarding these anouncements are free adverts.
The promise of information technologies in health care is another example. Its application is crucial for success, it is available, but it takes a long, long time to be applied. The disapointing impact of IT on health care has been the last year's article most read in Health Affairs . It is not by chance. We live in a society with a "too much technology" -TMT- syndrome. Organizations can't digest it without internal change in management and governance. Why not create some organizational conditions for success?
Each day every newspaper wants to convince us over a new technology. In biosciences, journalists enjoy talking about "opening doors" to new cures, and rarely anybody checks afterwards if this anouncement is really in place and provides its expected outcomes. Most of what we see in the media regarding these anouncements are free adverts.
The promise of information technologies in health care is another example. Its application is crucial for success, it is available, but it takes a long, long time to be applied. The disapointing impact of IT on health care has been the last year's article most read in Health Affairs . It is not by chance. We live in a society with a "too much technology" -TMT- syndrome. Organizations can't digest it without internal change in management and governance. Why not create some organizational conditions for success?
24 de gener 2014
Thrasymachus
Wikipedia dixit:
Quote from Plato's Thrasymachus in Republic I
Thrasymachus was a citizen of Chalcedon, on the Bosphorus. His career appears to have been spent as a sophist at Athens, although the exact nature of his work and thought is unclear. He is credited with an increase in the rhythmic character of Greek oratory, especially the use of the paeonic rhythm in prose, and a greater appeal to the emotions through gesture.
Quote from Plato's Thrasymachus in Republic I
338c: Ἄκουε δή, ἦ δ᾽ ὅς. φημὶ γὰρ ἐγὼ εἶναι τὸ δίκαιον οὐκ ἄλλο τι ἢ τὸ τοῦ κρείττονος συμφέρον..[1] (“Listen—I say that justice is nothing other than the advantage of the stronger.”)This forceful statement is dated from 426 BCE more or less. I'm just quoting it after 25 centuries.
Yesterday at Auditori. Jordi Savall and Le Concert des Nations. Impressive.
23 de gener 2014
Pharma news
The growth in the number of pharmaceutical prescriptions per capita in 2013 has fallen by 6,9%, unit price 1,8% less, and total expenditure minus 8,6%, completing a 4 years cycle of negative deelopment. This means that 80% of the decrease is due to the number of prescriptions.
It seems that physicians are increasing the quality of prescription following a specific policy. This is good news. However, more assessment is needed.
PS. Recent statement at Davos Conference:
"Europe's light at the end of the tunnel looks more and more like an oncoming train"
It seems that physicians are increasing the quality of prescription following a specific policy. This is good news. However, more assessment is needed.
PS. Recent statement at Davos Conference:
"Europe's light at the end of the tunnel looks more and more like an oncoming train"
21 de gener 2014
Where is the regulator?
Understanding the Economic Value of Molecular Diagnostic Tests: Case Studies and Lessons Learned
Maybe we have just arrived at the expected moment, when the cost of one whole genome sequencing is below $1000. (mapping up to 25.000 genes). At the same time, one test for 21 genes may cost you $4.500. This is our crazy world. In the first case you will only know your genome, in the second there will be a probability of success from a certain therapy.
There's only one question: Does anybody know any information about the reliability of such probabilities beyond the firm that is selling the test?. Where is the regulator?
After reading a recent article on the value of molecular diagnostic tests, I'm convinced that we still remain in an uncertain world in need of transparency. Given such uncertainty, better keep calm until the regulator confirms the clinical utility and cost-effectiveness of molecular diagnostic tests.
Maybe we have just arrived at the expected moment, when the cost of one whole genome sequencing is below $1000. (mapping up to 25.000 genes). At the same time, one test for 21 genes may cost you $4.500. This is our crazy world. In the first case you will only know your genome, in the second there will be a probability of success from a certain therapy.
There's only one question: Does anybody know any information about the reliability of such probabilities beyond the firm that is selling the test?. Where is the regulator?
After reading a recent article on the value of molecular diagnostic tests, I'm convinced that we still remain in an uncertain world in need of transparency. Given such uncertainty, better keep calm until the regulator confirms the clinical utility and cost-effectiveness of molecular diagnostic tests.
Parov Stelar Band - Jimmy's Gang (Unplugged in Moscow)
PS. You may avoid watching "The wolf of Wall Street" if you read this article.
15 de gener 2014
Poor quality regulation
Lyn Stout says in his book: Good laws makes good people. Today I would like to confirm again that bad regulation distorts markets. In 1999 it was decided that only group contracting for private health insurance would have some tax rebates, individual insurance lost such consideration. Fifteen years after, the government has decided that such rebates will be subject to social security contributions, this exactly means an increase in buyer's cost by 36%, 30% for the employer and 6% for the employee. In 2012 the average premium in the individual market was 731 €, while the group premium 562€. Such difference is huge since the product is nearly the same, and differential cost can't justify a discount of 23%. Former regulation may explain such distorsion, and precisely this was my argument in an article 3 years ago.
Nowadays group health insurance is not included under income tax, although it may be in the next step. Any government should assess how regulation distorts markets, and fit decisions to strictly improve markets functioning. I think that right now they are strictly thinking on more income and don't care about the impact that may be relevant next year.
Nowadays group health insurance is not included under income tax, although it may be in the next step. Any government should assess how regulation distorts markets, and fit decisions to strictly improve markets functioning. I think that right now they are strictly thinking on more income and don't care about the impact that may be relevant next year.
09 de gener 2014
On being accountable
FOCUSING ACCOUNTABILITY ON THE OUTCOMES THAT MATTER
A new report from a recent conference has been released. Accountable care is the term that summarises a US trend.
Beyond fashionable concepts, there is the reality. Let's take the definition for health care:
PS. Here you'll find an older post on the same topic of payment and incentives.
PS. Definition. Accountable. adjective \ə-ˈkau̇n-tə-bəl\ : required to explain actions or decisions to someone : required to be responsible for something
A new report from a recent conference has been released. Accountable care is the term that summarises a US trend.
Beyond fashionable concepts, there is the reality. Let's take the definition for health care:
Delivering accountable care for a population involves five key components:My impression is that in our health system we already have good examples of such organisations. Unfortunately, some issues fail due to wrong regulation. For example, payment and incentives, an issue that should be reformed as soon as possible.
1. A specified population for which providers are jointly accountable.
2. Target outcomes for the population - outcomes that matter to individuals.
3. Metrics and learning, to monitor performance on outcomes and to learn from variation.
4. Payments and incentives aligned with the target outcomes.
5. Co-ordinated delivery, across a range of providers, of the care necessary for
achieving the desired outcomes.
PS. Here you'll find an older post on the same topic of payment and incentives.
PS. Definition. Accountable. adjective \ə-ˈkau̇n-tə-bəl\ : required to explain actions or decisions to someone : required to be responsible for something
08 de gener 2014
The one and only option
Imagine for a moment a country, their citizens are presumably under the same constitution and tax law. Some citizens in a geographic area have a per capita public budget for health care for 2014 equal to 1.541 €. Other citizens, 1.091 € or less. There is no possible argument to maintain such huge and increasing differences. Is there any clever politician in the room to treat such disease? For sure, there isn't.
Simplistically speaking, my understanding is that we could decrease taxes by 28% or otherwise increase public health expenditures by 41%. Since these options are not plausible, the third is to forget such country because it is unable to solve the real public policy challenges. And worst than that, it obliges to apply budget cuts to those that already are spending less. Since such problems have persisted for three decades, the one and only option is to leave, reform is not a credible option.
PS. Data
Simplistically speaking, my understanding is that we could decrease taxes by 28% or otherwise increase public health expenditures by 41%. Since these options are not plausible, the third is to forget such country because it is unable to solve the real public policy challenges. And worst than that, it obliges to apply budget cuts to those that already are spending less. Since such problems have persisted for three decades, the one and only option is to leave, reform is not a credible option.
PS. Data
Subscriure's a:
Missatges (Atom)