The Hungry Gene. The Inside Story of the Obesity Industry

VALUES, ETHICS AND HEALTH CARE
Peter Duncan dixit:
We develop health care, and fund health care systems, broadly so that we can improve health. This very wide conception of the ends of health care leads us back to the kinds of things that Edwards mentions. From these, we can perhaps suggest that the values central to health care include things like autonomy (associated with further values such as free will, respect and consent), caring (also involving compassion and responsibility) and equality (which might also include values of justice and fairness).

A low incidence of catastrophic expenses sometimes reflects low service coverage (often in low-income countries) but sometimes occurs despite high service coverage (often in high-income countries). At a given level of service coverage, financial protection also varies. UHC index scores are generally higher in higher-income countries, but there are variations within income groups. Adjusting the UHC index for inequality in service coverage makes little difference in some countries, but reduces it by more than 10% in others. Seven of the 12 countries for which we were able to produce trend data have increased their UHC index over time (with the greatest average yearly increases seen in Ghana [1·43%], Indonesia [1·85%], and Vietnam [2·26%]), mostly by improving both financial protection and service coverage. Some increased their UHC index, despite reductions in financial protection, by substantially increasing their service coverage. The UHC index decreased in five of 12 countries with trend data, mostly because financial protection worsened with stagnant or declining service coverage. Our UHC indicators (except inpatient admissions) are significantly and positively associated with GDP per capita, and most are correlated with the share of health spending channelled through social health insurance and government schemes. However, associations of our UHC indicators with the share of GDP spent on health and the shares of health spending channelled through non-profit and private insurance are ambiguous.
Great article by Wagstaff and Neelsen.
Overcoming the Market Dominance of Hospitals
The facts:
Consolidation has been a predominant business strategy for hospitals and physicians in the United States for decades. Hospitals consolidate to gain market share and use resulting leverage to charge higher prices to private payers or employers large enough to self-insure. One major reason this may occur with relatively little resistance is the nature of health care markets. Numerous plans compete to offer health insurance to employers, and employers that self-insure must select from among these plans or third-party administrators (TPAs).
To attract employers, payers and TPAs strive to offer large networks of clinicians and health care centers to minimize care disruptions for employees. But when most physicians in a region are employed by a large hospital network, private payers and employers often have limited options other than to contract with that network, forcing them to tolerate 6% to 10% increases in prices each year.7 Adding to their leverage, these large networks often offer differentiated services like organ transplants or advanced specialty therapies that make them a “must-have” in private-payer or employer networks. Thus, the financial incentive for hospitals to merge or acquire physicians to gain must-have status is high.
Hospital consolidation is also supported by the nature of antitrust regulations, which are limited by how markets are defined. Since the 1990s, academics and regulators have defined local markets in health care using tertiary hospital catchment areas or hospital referral regions (HRRs). HRRs were constructed based on referral patterns of cardiovascular and neurosurgery hospitalizations from 1992-1993 Medicare data for research purposes.8 Yet these outdated HRRs meant for research are frequently used in antitrust enforcement today, despite the hospital mergers that have occurred since their development. In 2018, a review of community hospitals reported that 3491 of 5198 hospitals (67%) belonged to a multihospital health system, compared with just 2524 of 4956 (51%) in 1998.
Take-away message:
COVID-19 has the potential to exacerbate the nation’s history of hospital consolidation. Stronger incentives to counteract consolidation could protect patients against potential adverse effects of anticompetitive hospital networks. Policy makers and regulators should consider legislation that defines and regulates market-dominant hospitals MDHs, while promoting asset redistribution via market-dominant hospitals redistribution fund MRF, as a potential safeguard to the adverse consequences of the consolidation trend

HBR's 10 Must Reads on Platforms and Ecosystems
This collection of articles includes "Pipelines, Platforms, and the New Rules of Strategy," by Marshall W. Van Alstyne, Geoffrey G. Parker, and Sangeet Paul Choudary; "Strategies for Two-Sided Markets," Thomas R. Eisenmann, Geoffrey Parker, and Marshall W. Van Alstyne; "Finding the Platform in Your Product," by Andrei Hagiu and Elizabeth Altman; "What's Your Google Strategy?," by Andrei Hagiu and David B. Yoffie; "In the Ecosystem Economy, What's Your Strategy? ," by Michael G. Jacobides; "Right Tech, Wrong Time," by Ron Adner and Rahul Kapoor; "Managing Our Hub Economy," by Marco Iansiti and Karim R. Lakhani; "Why Some Platforms Thrive and Others Don't," by Feng Zhu and Marco Iansiti; "Spontaneous Deregulation," by Benjamin Edelman and Damien Geradin; "Alibaba and the Future of Business," by Ming Zeng; and "Fixing Discrimination in Online Marketplaces," by Ray Fisman and Michael Luca.
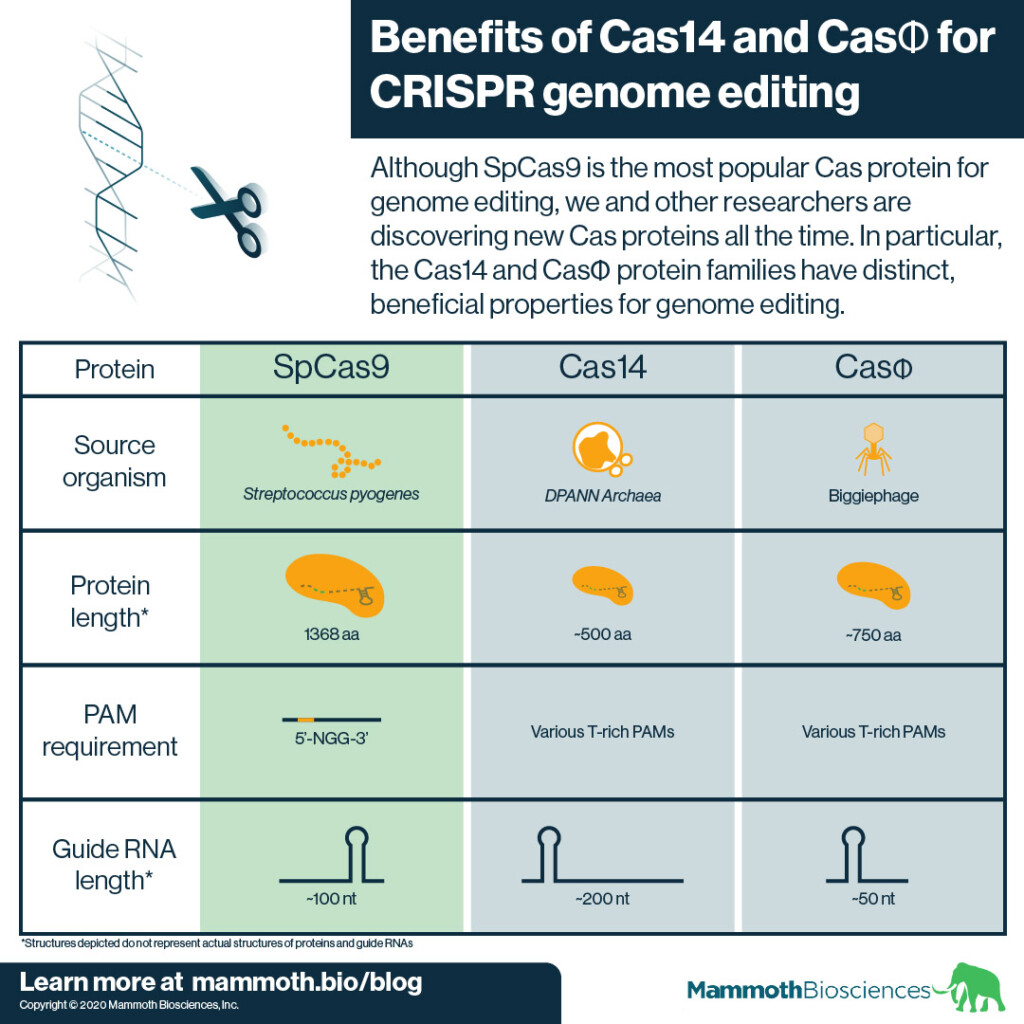
Expanding the possibilities of CRISPR genome editing with Cas14 and CasΦ
SpCas9 comes from a bacterium called Streptococcus pyogenes (hence “Sp”). S. pyogenes is a human pathogen. There is some evidence that using SpCas9 for genome editing in humans may lead to dangerous immune reactions (Ferdosi et al 2019) although other reports have questioned the importance of this finding.
In addition SpCas9 is quite large. It is 1368 amino acids (aa) long and can be difficult to fit into standard delivery vehicles (learn about CRISPR delivery here). Thus it can be hard to get SpCas9 into target cells and tissues.
Finally, SpCas9 requires the presence of a specific DNA sequence known as a “PAM” to target an adjacent sequence for genome editing. SpCas9’s PAM is 5’-NGG-3’. The need for this sequence restricts the number of sites SpCas9 can edit. This limits SpCas9’s usefulness.
Skills for the future health workforce: Preparing health professionals for people centred care
This is the focus of the OECD paper:
This paper discusses transversal (core) skills that are required by health professionals for a successful transition from fragmented and disease-centred care towards people-centred healthcare delivery systems. The discussion is motivated by the growing evidence of skills mismatch among health professionals. These transversal skills include interpersonal skills, such as person-centred communication, interprofessional teamwork, self-awareness and socio-cultural sensitivity, as well as analytical skills, such as adaptive problem solving to devise customised care for individual persons, system thinking, openness to continuous learning, and the ability to use digital technologies effectively
Sounds of interest. However, it forgets a key issue. Life sciences are changing and knowledge breaks barriers that gave birth to excessive specialization. Therefore, more issues to add in the next future.

Opportunities and challenges in long-read sequencing data analysis
Long reads: their purpose and place
Long-read sequencing, or third-generation sequencing, offers a number of advantages over short-read sequencing. While short-read sequencers such as Illumina’s NovaSeq, HiSeq, NextSeq, and MiSeq instruments; BGI’sMGISEQand BGISEQmodels; or ThermoFisher’s Ion Torrent sequencers produce reads of up to 600 bases, long-read sequencing technologies routinely generate reads in excess of 10 kb
Long-read technologies are improving rapidly, and may become the mainstay of sequencing; however, the broader application of long-read technologies are currently limited by a lower throughput, higher error rate and higher cost per base relative to short read sequencing. Wider use of such technologies in the clinical context may rapidly improve our understanding of cancer, pathogen evolution, drug resistance and genetic diversity in complex regions of the genome that have important implications for clinical care. Parallel development of existing technology to allow high throughput PCR-free sequencing will be important in sequencing difficult regions of the genome.
At present, no single long-read technology has any clear advantage from a scientific point of view, and thus it seems likely that the future of long-read sequencing is more likely to be decided on commercial terms rather than scientific. Whichever technology captures the market, it is clear that as these technologies become more affordable they will continue to shine a light into previously intractable regions of the genome with ever larger sample sizes and longer read-lengths, allowing new discovery in these evolving fields.
Just looking at stock exchange you may confirm that the decision is being made in commercial terms. It seems that there is a role for a cost-effectiveness evaluation right now.

Robert Frank, València 1952
Mort amb recepta (catalan version)
Annual report on Drugs in Catalonia (p.152)
Oxicodone in Catalonia: from 879.775 DDD in 2014 to 1.003.355 in 2019, a 14% increase. Tramadol: from 11.790.547 DDD in 2014 to 17.038.936 in 2019, a 69% INCREASE in 5 YEARS (p.152)
Daily Dose per Inhabitant (DDH)Tramadol: from 4,27 to 6,16 a 44,2% INCREASE in 5 YEARS
A worrying french situation
The documentary: Etats-Unis, la mort sur ordonnance
Nan Goldin denounces: Who profits form the opioid crisis?

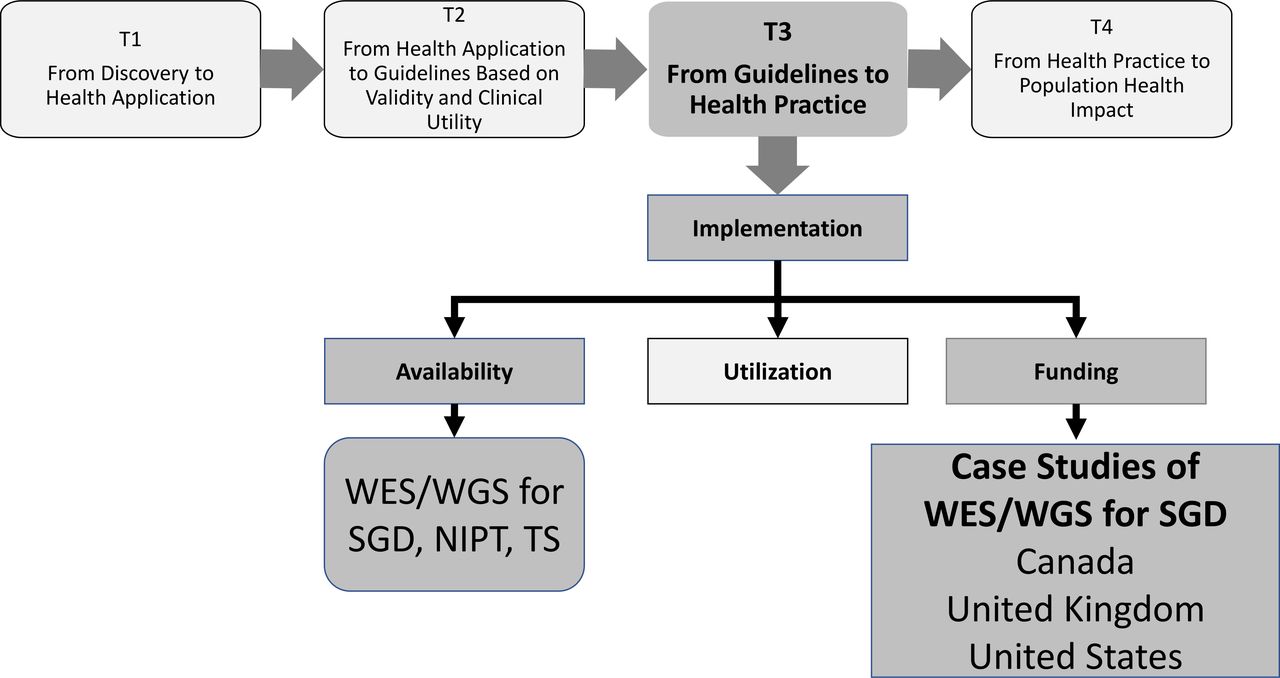
Availability and funding of clinical genomic sequencing globally
A useful review on the current situation:
Our case studies, based on published and unpublished literature as well as discussions with key experts in each country, are illustrative of three types of funding systems:
Publicly funded/national system: UK, which is one of a few countries with national, government-based funding for NGS (others include Belgium, Denmark, the Netherlands and Australia).
Publicly funded/provincial system: Canada, for which public funding of tests is provided at the provincial level after approval based on meeting specific criteria.
Mixed private/public system: USA, which has variable private and public insurer coverage.
The 4 steps: