Morbilidad, utilización de recursos y costes sanitarios en la comarca del Baix Empordà
In this blog I've explained many times that if I had to pick one health system as a benchmark I would say that it is Serveis Sanitaris Integrats del Baix Empordà (SSIBE). This is my choice. I've been contributing over the last decade to understand what has happened to the morbidity, utilization and costs of this population.
Now, you have all this research effort in a PhD Dissertation by J. M. Inoriza, a must read. I strongly recommend you to have a look at it. Congratulations to all contributors.
26 de setembre 2015
25 de setembre 2015
Health policy: what works?
Successes and Failures of Health Policy in Europe. Four decades of divergent trends and converging challenges
Three questions to answer:
The book was released in 2013 with data from 5 years before, an update would be necessary. Anyway, a close reading is required.
Three questions to answer:
- Do differences in rates of disease reflect differences in related policies?
- What would a country gain if it implemented the policies of the best performing country?
- Which social, economic and political factors influence a country's success in health policy?
Gains in health since 1970 for the causes analysed in this chapter have clearly been enormous. While not all of these declines can be attributed to health policies, part of the decline in all these causes can be, as shown in the previous chapters. For example, some of the declines in lung cancer and ischaemic heart disease can be attributed to tobacco control; some of the declines in external cause mortality among children to injury prevention, and some of the declines in death rate from RTIs to road safety measures, and so on. It is impossible to estimate the specific contribution of preventive health policies to these declines, but even if these accounted for only half or a quarter of the cause-specifi c declines, the successes would be immense. At the same time, not all countries have been equally successful in bringing down mortality from these preventable causes, as shown again by the calculations.
The book was released in 2013 with data from 5 years before, an update would be necessary. Anyway, a close reading is required.
24 de setembre 2015
The modeling approach to health decisions
Applying Modeling to Improve Health and Economic Policy Decisions in the Americas: The Case of Noncommunicable Diseases
On the role of modeling in health, this OECD report says:
PS. An innovative approach with practical implications in SSIBE, Palamós.

On the role of modeling in health, this OECD report says:
In the health sector, the purpose of modeling is to structure evidence on clinical and economic outcomes in a form that can inform decisions about clinical practices and health care resource allocations. Models synthesize evidence on health consequences and costs from many different sources, including clinical trials, observational studies, insurance claim databases, case registries, public health statistics, and preference surveys. A model’s logical, mathematical framework permits the integration of facts and values and links these data to outcomes that are of interest to health care decisionmakersI agree. The report shows some examples of aggregated modeling without panel microdata. If you compare this approach with David Eddy one, Archimedes models, it is exactly the opposite. And my opinion is in favour of Archimedes, as you can check in my previous posts. The most useful approach to modeling is the one that allows improve decisions at micro level, physician and patient.
PS. An innovative approach with practical implications in SSIBE, Palamós.

Bonnard exhibition in Madrid.
19 de setembre 2015
The size of income inequality (2)

17 de setembre 2015
Epigenetics contribution to clarify disease mechanisms
Epigenetics at the Crossroads of Genes and the Environment
You may find an updated definition of epigenetics in this JAMA article:
PS. Epigenetic phenomena, from Nature.
You may find an updated definition of epigenetics in this JAMA article:
Epigenetics refers to information transmitted during cell division other than the DNA sequence per se, and it is the language that distinguishes stem cells fromIf this is so, why is the message of predictive genetics so widespread?. I've insisted on this issue before.
somatic cells, one organ from another, and even identical twins from each other. Examples include (1) DNA methylation, a covalent modification of the nucleotide cytosine, that is copied during cell division at CpG dinucleotides by the maintenance enzyme DNA methyltransferase I; (2) posttranslational modifications of nucleosome proteins about which the DNA double helix is wrapped; and (3) the density of nucleosomes and higher-order packaging of chromatin within the nucleus, including its relationship to the nuclear lamina.
The field of epigenetics and epigenetic epidemiology have much to do to improve measurement of epigenetic marks, inform natural variation in such marks, and the biological and population level relationships between genes, environment, and epigenetics. This is an important emerging area as it holds promise for better risk prediction in precision medicine as well as for clarification of disease mechanisms among the existing opaque landscape only partially informed by traditional genetic and environmental studies to date.A short and relevant article that provides hints for further reading.
PS. Epigenetic phenomena, from Nature.
16 de setembre 2015
Ownership and access to medical data
Unpatients—why patients should own their medical data
Eric Topol says in Nature Biotechnology:
PS. Hacking electronic records:
 The timeline for electronic medical data hacks in the United States of over 1 million individuals
The timeline for electronic medical data hacks in the United States of over 1 million individuals
Eric Topol says in Nature Biotechnology:
Today, in the United States, health data live in a plethora of places, from electronic health record (EHR) systems, insurance claims databases, siloed personal health apps, research and clinical trial databases, imaging files and lots of paper. Although seemingly everywhere, any true semblance of an overarching organization or standardization of medical data are lacking, whether at the individual or societal levelHis proposal is straightfoward: the ownership of the clinical record is of the patient. This situation is completely different in our country. We have public centralised repositories and the patient is the owner. There is still a lack of coordination and many things to solve, however the basics are covered in the publicly funded System, that's not the case in the private sector.
In contrast to the legal and technical difficulty an individual faces to obtain all his or her own medical data is the relative ease with which hackers have managed to breach ~100 million patient records in the first half of 2015And his proposal:
We must begin talking about creating a health data resource in a much broader and more universal context, controlled by the individuals who supply the data. This is a unique moment where we may be able to provide for personal control and, at the same time, create a global knowledge medical resource.Sounds interesting, though methodology is crucial for success.
PS. Hacking electronic records:

04 de setembre 2015
Cardiovascular disease and diabetes: progress and prospects
OECD Health Policy Studies Cardiovascular Disease and Diabetes
A recent OECD report highlights the huge improvement on cardiovascular disease and at the same time explains the policies and strategies needed for the near future. Treatment improvement accounts for 40% in the decrease of mortality, change in risk factors 50%, while 10% is unexplained. This means that public policy is critical for success. Nowadays it is still the first disease to tackle. On diabetes, the report explains that 85 million europeans are currently suffering from the disease. Therefore, it remains a severe issue.
I suggest you take a close look at the report.
A recent OECD report highlights the huge improvement on cardiovascular disease and at the same time explains the policies and strategies needed for the near future. Treatment improvement accounts for 40% in the decrease of mortality, change in risk factors 50%, while 10% is unexplained. This means that public policy is critical for success. Nowadays it is still the first disease to tackle. On diabetes, the report explains that 85 million europeans are currently suffering from the disease. Therefore, it remains a severe issue.
I suggest you take a close look at the report.
28 d’agost 2015
Healthy life expectancy: the key indicator
Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: quantifying the epidemiological transition
In former posts I have advocated that healthy life expectancy should be used as an aggregated indicator of outcomes of health determinants. Unfortunately although it is imperfect, it is the best we have, and today you can check the latest estimates in a salient article in The Lancet.
Countries with highest healthy life expectancy, both sexes, 2013
Spain has disappeared from the former top 10. I have always said that ordinal rankings have flaws, however, comparisons across time are worth taking into account.
Internally in Spain it is difficult to reverse this trend. If you consider geographic variations of the indicator you can see a range from 55 years up to 65 (p.25) .Therefore there is too much noise when you focus on the state as the unit of analysis. Forget the results and the ranking.
The only situation that is unique in the ranking is Andorra, it always appear at the top and it is a small state. That's remarkable and merits close analysis.

In former posts I have advocated that healthy life expectancy should be used as an aggregated indicator of outcomes of health determinants. Unfortunately although it is imperfect, it is the best we have, and today you can check the latest estimates in a salient article in The Lancet.
Countries with highest healthy life expectancy, both sexes, 2013
| 1 | Japan |
| 2 | Singapore |
| 3 | Andorra |
| 4 | Iceland |
| 5 | Cyprus |
| 6 | Israel |
| 7 | France |
| 8 | Italy |
| 9 | South Korea |
| 10 | Canada |
Spain has disappeared from the former top 10. I have always said that ordinal rankings have flaws, however, comparisons across time are worth taking into account.
Internally in Spain it is difficult to reverse this trend. If you consider geographic variations of the indicator you can see a range from 55 years up to 65 (p.25) .Therefore there is too much noise when you focus on the state as the unit of analysis. Forget the results and the ranking.
The only situation that is unique in the ranking is Andorra, it always appear at the top and it is a small state. That's remarkable and merits close analysis.

26 d’agost 2015
Beware of healthcare providers consolidation
The Potential Hazards of Hospital Consolidation Implications for Quality, Access, and Price
The key message:
The key message:
With the current most substantial consolidation of health care in US history, the concerning implications of the trend of hospital consolidation on quality, access, and price must be carefully considered. However, unlike banks that became too big to fail, 85% of US hospitals pay no taxes because they are designated as nonprofit organizations serving a public good. Hospitals can set prices that are ultimately passed on to others in the form of escalating insurance deductibles and taxes.The alternative:
The good work of integrated hospitals should continue to create networks of coordinated care, while at the same time, physicians and patients should insist that hospitals compete on transparent prices and quality outcomes. Achieving this goal is an important prerequisite to a functional health care system.
25 d’agost 2015
Tackling obesity: the toolbox
Patchy progress on obesity prevention: emerging examples, entrenched barriers, and new thinking
World Cancer Research Fund International NOURISHING framework
Food policy framework for healthy diets and the prevention of obesity and diet-related non-communicable diseases.

Key message:

World Cancer Research Fund International NOURISHING framework
Food policy framework for healthy diets and the prevention of obesity and diet-related non-communicable diseases.

Key message:
The problem of obesity must be reframed to acknowledge on one hand that individuals bear some personal responsibility for their health, but that, on the other hand, environmental factors exploit biological, psychological, social, and economic vulnerabilities that promote overconsumption of unhealthy foods. A vicious cycle is created in which the preference and demand for unhealthy products are not only shaped by the environment, but lead to environmental changes that further encourage consumption of unhealthy foods. This cycle makes it difficult for people to act in their own long-term self-interest, but it can be broken with regulatory actions from governments and joint efforts from industry and civil society to create healthier food systems.

07 d’agost 2015
European health regulation on lab tests, the final round?
Medical devices: Council getting ready for talks with EP
Last June 15th, there was a small but significant step towards the final agreement on Medical devices and in vitro diagnostics regulation in Europe. The need for reform has been widely requested but the lack of political consensus and the low priority given to the issue has delayed its approval in many ocasions. It seems that now is the right opportunity, however if finally passes, it will be applied on 2020!!!. It really sounds weird that it would take 5 years to be fully developed.
Anyway, if you want to have a look at the details check here and here. Right now, the lobbies are not on vacation, they are fighting against some provisions that limit their current freedom of market access. Pay attention to final result, just to check who wins and who loses, and the current state of power balance between society and the lobbies.

Last June 15th, there was a small but significant step towards the final agreement on Medical devices and in vitro diagnostics regulation in Europe. The need for reform has been widely requested but the lack of political consensus and the low priority given to the issue has delayed its approval in many ocasions. It seems that now is the right opportunity, however if finally passes, it will be applied on 2020!!!. It really sounds weird that it would take 5 years to be fully developed.
Anyway, if you want to have a look at the details check here and here. Right now, the lobbies are not on vacation, they are fighting against some provisions that limit their current freedom of market access. Pay attention to final result, just to check who wins and who loses, and the current state of power balance between society and the lobbies.

NESBITT, Lowell. Dos ponts a Nova York, 1975
06 d’agost 2015
The size of income inequality
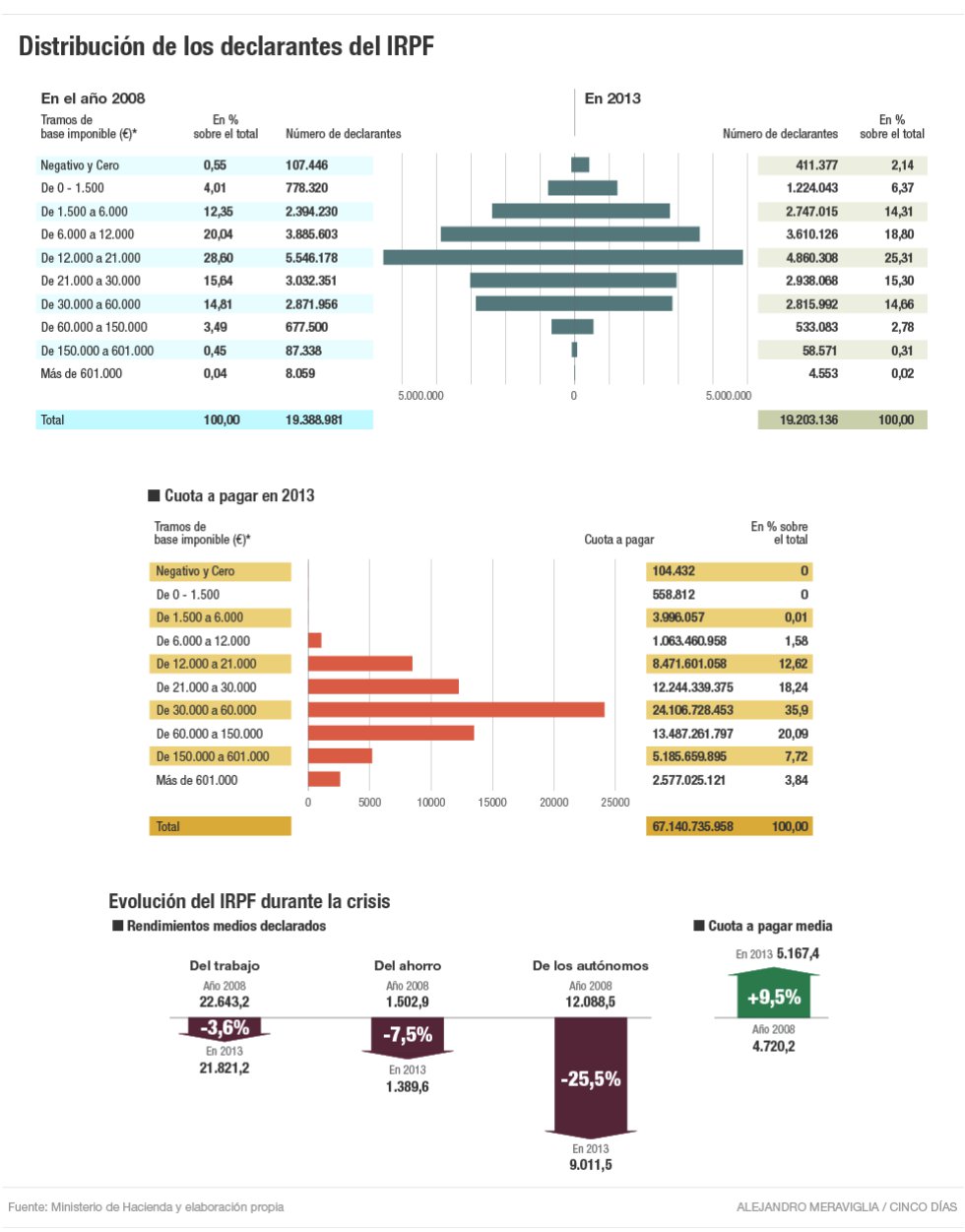
Income declared to tax authorities, not actual income. Selected statements:
- 3% of citizens account for 30% of tax collection!
- In 5 years, plutocrats have decreased by 50%!
- In 5 years, average work income has plummeted 3,6% and taxes jumped to 9,5%!
My congratulations, tax authorities!
05 d’agost 2015
04 d’agost 2015
Stratified medicine: defining the size of the market
Trusheim and Berndt provide an excellent overview of the economics of stratified medicine. I have reviewed the topic before and specifically in this post. An ideal companion diagnostic perfectly identifies and distinguishes treatment responders from those who will not.Unfortunately, in practice no diagnostic performs ideally. All diagnostics experience some level of error. In the case of a companion diagnostic, some patients will receive false positive results, scores indicating they will respond, but will not when treated. Other patients will receive false negative results, scores indicating they will not respond, but if treated they would.
So what? The key issue is about the setting of the cut-off that will define the size of the market:
Under competition, three essentially identical drugs may receive dramatically different labels, incremental cost-effectiveness ratio (ICER) justified pricing, and market positioning depending on their stratification approach. It appears superior to use an imperfect biomarker to none at all. It is less obvious whether patients, payers and firms prefer the same cut-off values for the companion diagnostic, or even whether each stakeholder a priori prefers the high, low or perhaps some other CDx cut-off value.The implications for regulating and financing of companion diagnostics are immediate. In Europe current legislation is as old as of 1998, the year that Herceptin entered into the market and the begining of stratified medicine. New regulation is still pending and there are no perspectives about a unified approach to lab tests assessment. European regulator is still on vacation.
The competing development teams may face a version of the game theory ‘prisoner’s dilemma’ in which the optimal result for patients and all firms would be to select a low or mid companion diagnostic cut-off value but the advantages of a potentially differentiating high efficacy claim may drive developers to select a high cut-off value. If all choose this approach, overall value may be reduced with many patients excluded from treatment. But the potential advantage of a higher cut-off value may prove too alluring, or the fear of a competitor selecting one, may drive all to do so. Each situation will depend on the specific facts of the indication, therapeutic, companion diagnostic and competitors
Subscriure's a:
Missatges (Atom)