Long time ago I alerted about a potential payment system that tried to convince everybody and didn't satisfied its goals for equity and efficiency. I was concerned about reproducing the mistakes of the past and creating flaws for the future. What I said more than two years ago, has been recently confirmed more or less by a recent decree. Its detailed analysis goes beyond any post in a blog. The retro part is related to an administrative discretionary classification of hospitals that was initially defined two decades ago (Decree June 30th, 1992) and failed afterwards. The future part is related to a dual payment system: population and service based that will be defined according to idiosyncratic situations. Both are the pillars of uncertainty in the model.
Right now the most important task to accomplish will be to think about its next reform.
Es mostren les entrades ordenades per rellevància per a la consulta uncertainty. Ordena per data Mostra totes les entrades
Es mostren les entrades ordenades per rellevància per a la consulta uncertainty. Ordena per data Mostra totes les entrades
09 de setembre 2014
01 de febrer 2019
Medicine as a data science (3)
High-performance medicine: the convergence of human and artificial intelligence
If you want to know the current state of artificial intelligence in medicine, then Eric Topol review in Nature is the article you have to read. A highlighted statement:
Therefore, take care when you look at tables like this one:
If you want to know the current state of artificial intelligence in medicine, then Eric Topol review in Nature is the article you have to read. A highlighted statement:
There are differences between the prediction metric for a cohort and an individual prediction metric. If a model’s AUC is 0.95, which most would qualify as very accurate,And this is good summary:
this reflects how good the model is for predicting an outcome, such as death, for the overall cohort. But most models are essentially classifiers and are not capable of precise prediction at the individual level, so there is still an important dimension of uncertainty.
Despite all the promises of AI technology, there are formidable obstacles and pitfalls. The state of AI hype has far exceeded the state of AI science, especially when it pertains to validation and readiness for implementation in patient care. A recent example is IBM Watson Health’s cancer AI algorithm (known as Watson for Oncology). Used by hundreds of hospitals around the world for recommending treatments for patients with cancer, the algorithm was based on a small number of synthetic, nonreal cases with very limited input (real data) of oncologists. Many of the actual output recommendations for treatment were shown to be erroneous, such as suggesting the use of bevacizumab in a patient with severe bleeding, which represents an explicit contraindication and ‘black box’ warning for the drug. This example also highlights the potential for major harm to patients, and thus for medical malpractice, by a flawed algorithm. Instead of a single doctor’s mistake hurting a patient, the potential for a machine algorithm inducing iatrogenic risk is vast. This is all the more reason that systematic debugging, audit, extensive simulation, and validation, along with prospective scrutiny, are required when an AI algorithm is unleashed in clinical practice. It also underscores the need to require more evidence and robust validation to exceed the recent downgrading of FDA regulatory requirements for medical algorithm approval
Therefore, take care when you look at tables like this one:
| Prediction | n | AUC | Publication (Reference number) |
|---|---|---|---|
| In-hospital mortality, unplanned readmission, prolonged LOS, final discharge diagnosis | 216,221 | 0.93* 0.75+0.85# | Rajkomar et al.96 |
| All-cause 3–12 month mortality | 221,284 | 0.93^ | Avati et al.91 |
| Readmission | 1,068 | 0.78 | Shameer et al.106 |
| Sepsis | 230,936 | 0.67 | Horng et al.102 |
| Septic shock | 16,234 | 0.83 | Henry et al.103 |
| Severe sepsis | 203,000 | 0.85@ | Culliton et al.104 |
| Clostridium difficile infection | 256,732 | 0.82++ | Oh et al.93 |
| Developing diseases | 704,587 | range | Miotto et al.97 |
| Diagnosis | 18,590 | 0.96 | Yang et al.90 |
| Dementia | 76,367 | 0.91 | Cleret de Langavant et al.92 |
| Alzheimer’s Disease ( + amyloid imaging) | 273 | 0.91 | Mathotaarachchi et al.98 |
| Mortality after cancer chemotherapy | 26,946 | 0.94 | Elfiky et al.95 |
| Disease onset for 133 conditions | 298,000 | range | Razavian et al.105 |
| Suicide | 5,543 | 0.84 | Walsh et al.86 |
| Delirium | 18,223 | 0.68 | Wong et al.100 |
03 de març 2021
The inescapable architecture of everyday life
Choice Architecture. A New Approach to Behavior, Design, and Wellness
The contents of the book:
1 The Inescapable Architecture of Everyday Life
2 A Framework for Architectural Interpretation
2.1 Rational Persons
2.2 Architects and Designers
2.3 Looking a Little More Closely at What Happens Inside Phil
2.6 The Architectural Problem
2.7 Phil Can Sometimes be Inconsistently Rational
2.8 How Tom’s Irrationality can Sometimes Help Him
2.9 The Architectural Problem Revisited
3 Rational and Irrational Behavior
3.1 Back to Consistent Rationality
3.2 Anchoring
3.3 Availability
3.4 The Cost of Zero Cost
3.5 Nonlinearity
3.6 Representativeness
3.7 Framing
3.8 Reference Point Shifts
3.9 An Overview of the Architectural Problem
4. Reflecting on choice architecture
4.1 Choice architecture is not a tree
4.2 The Structure of Architectural Experience
4.3 A Few Cautionary Remarks
4.4 Uncertainty

12 d’agost 2018
Searching for principles to inform societal decisions
Health Economics from Theory to Practice: Optimally Informing Joint Decisions of Research, Reimbursement and Regulation with Health System Budget Constraints and Community Objectives
Cost effectiveness analysis without a clear understanding of budget impact is a theoretical effort with limited consequences in practice. If you want a clear view of the whole process and go beyond cost-effectiveness, a new book tries to summarise the current state of the art.
I'm not so sure that the title "Health economics from theory to practice" really fits with content you expect, but think about a different title "cost-effectiveness from theory to practice" and this is precisely what you'll find.

Cost effectiveness analysis without a clear understanding of budget impact is a theoretical effort with limited consequences in practice. If you want a clear view of the whole process and go beyond cost-effectiveness, a new book tries to summarise the current state of the art.
I'm not so sure that the title "Health economics from theory to practice" really fits with content you expect, but think about a different title "cost-effectiveness from theory to practice" and this is precisely what you'll find.
This book provides a robust set of health economic principles and methods to inform societal decisions in relation to research, reimbursement and regulation (pricing and monitoring of performance in practice). We provide a theoretical and practical framework that navigates to avoid common biases and suboptimal outcomes observed in recent and current practice of health economic analysis, as opposed to claiming to be comprehensive in covering all methods. Our aim is to facilitate efficient health system decision making processes in research, reimbursement and regulation, which promote constrained optimisation of community outcomes from a societal perspective given resource constraints, available technology and processes of technology assessment. Importantly, this includes identifying an efficient process to maximize the potential that arises from research and pricing in relation to existing technology under uncertainty, given current evidence and associated opportunity costs of investment. Principles and methods are identified and illustrated across health promotion, prevention and palliative care settings as well as treatment settings. Health policy implications are also highlighted.And the conclusion:
The framework and methods presented have been shown to enable optimising of joint research, reimbursement (adoption and financing) and regulatory (pricing and practice monitoring) processes and decision making. Jointly addressing these related decisions has been shown to be key in meeting current and future challenges of baby boomer ageing and more generally in identifying areas for policy reform to enable a pathway to budget-constrained optimisation of community net benefit. The bottom line for such reforms is that better use of existing programmes and technologies and associated research that reflect community preferences is required and particularly now in facing the challenge of budget-constrained successful ageing of the baby boomer cohort.
07 de setembre 2016
A healthcare expenditure mess, and nobody cares about it
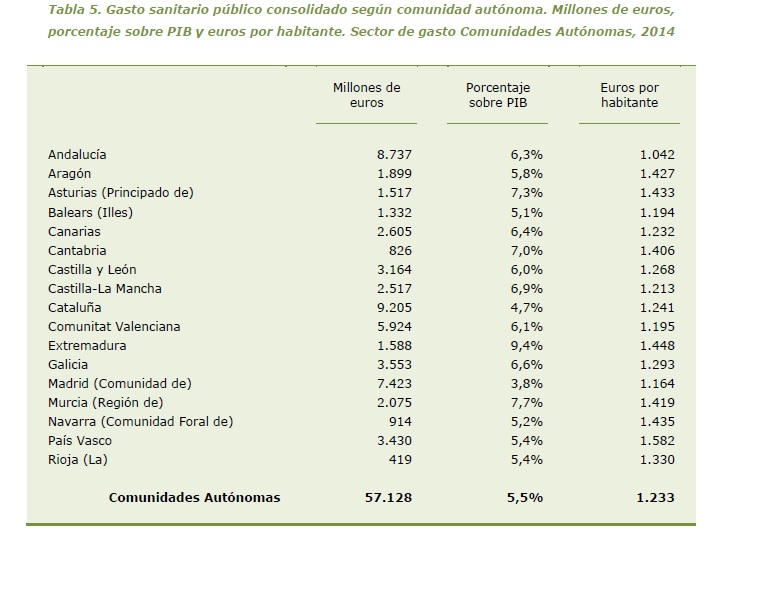
Let's imagine an alleged State. All its citizens pay taxes under the same Tax Code. Health Benefits are the same under the Health Act. And spending on health care according to geography, can reach 52% more in Basque country compared to Andalusia. This is not new. Many decades having the same figure and nobody cares about it.
 This is an easy table to understand health policy making in a failed state. Catalonia spends 4,7% of GDP on health, other sources say 5,5%. Anyway, you'll not find an OECD country with similar figures. After a decade we are spending the same amount per citizen than in 2006, 1.120 €. I will not add anything to this mess. There is only an increasing need to disconnect. Is there any MP in the room?
This is an easy table to understand health policy making in a failed state. Catalonia spends 4,7% of GDP on health, other sources say 5,5%. Anyway, you'll not find an OECD country with similar figures. After a decade we are spending the same amount per citizen than in 2006, 1.120 €. I will not add anything to this mess. There is only an increasing need to disconnect. Is there any MP in the room?
 This is an easy table to understand health policy making in a failed state. Catalonia spends 4,7% of GDP on health, other sources say 5,5%. Anyway, you'll not find an OECD country with similar figures. After a decade we are spending the same amount per citizen than in 2006, 1.120 €. I will not add anything to this mess. There is only an increasing need to disconnect. Is there any MP in the room?
This is an easy table to understand health policy making in a failed state. Catalonia spends 4,7% of GDP on health, other sources say 5,5%. Anyway, you'll not find an OECD country with similar figures. After a decade we are spending the same amount per citizen than in 2006, 1.120 €. I will not add anything to this mess. There is only an increasing need to disconnect. Is there any MP in the room?
PS. I'm not arguing that every country has to spend the same, I'm just saying that it is not legally possible to deliver the same benefits with such different budgets. Therefore we are unequal before law. This is the usual legal uncertainty of a failed state.
20 de març 2013
P4P: Ethics and effectiveness
Ethical Physician Incentives — From Carrots and Sticks to Shared Purpose
The strict focus on carrots and sticks in the design of physician incentives may contribute to unintended results. Have a look at NEJM and you'll find an outstanding article that puts the stuff in the right place:
PS. On the HA blog you'll find the same topic and the same conclusion, by Dan Arieli and Stephie Woolhandler:
The strict focus on carrots and sticks in the design of physician incentives may contribute to unintended results. Have a look at NEJM and you'll find an outstanding article that puts the stuff in the right place:
Using incentives both effectively and ethically requires a shift away from a simple, one-lever model that relies on tradition, self-interest, or emotional responses to reward participants for a desired action (or punish them with financial loss or shame for an undesired one). Such an approach risks alienating physicians and other personnel. Rather, the challenge is to cultivate consensus on an organization’s shared purpose and put that orientation into action through performance measurement and use of the other types of incentives.However, having said that, we know that the introduction of performance measures may be easier than to create a shared-purpose orientation on the organization (i.e. "an organizational commitment to the triple aim of improved patient outcomes, better population health and efficient costs"). Therefore, there is a need to guarantee "ethical conditions" under any pay-for-performance (P4P) scheme. Although I agree absolutely in this approach, the precondition is a consensus in the whole organization, from the top (board of directors) to the bottom (employees) and I'm uncertain about how to build and create such consensus in the current environment. Anyway, such uncertainty should not prevent efforts in this direction.
PS. On the HA blog you'll find the same topic and the same conclusion, by Dan Arieli and Stephie Woolhandler:
None can doubt health care’s grave quality deficits and cost excesses. As remedy, P4P suggests manipulating greed, a fuel that’s powered exponential growth in productivity in the overall economy. But Adam Smith, who first recognized greed’s awesome power, was also a moral philosopher who believed that commodity production required a parallel public service economy driven by social duty.
Sadly, greed has caused many of the worst abuses within the current system. Injecting different monetary incentives into health care can certainly change it, but not necessarily in the ways that policy makers would plan, much less hope for.
28 de setembre 2011
La part plana de la corba
Flat-of-the-curve medicine: a new perspective on the production of health
Aquest estiu s'ha estrenat una nova revista d'economia de la salut "Health Economics Review". Aquesta és una bona notícia i té alhora una novetat destacable, és en accés obert. Un dels primers articles que han sortit ha estat el d'en Zweifel i Shoder que es pregunten en termes agregats si en treiem alguna cosa a canvi de la despesa addicional en assistència sanitària que fem. Dit altrament, si en termes marginals, més recursos han aportat més salut. Llegiu-lo sencer, no hi ha excusa, l'accés és obert. Destaco paràgrafs clau:
PS. Ahir es va anunciar al Parlament que hi ha un país que l'any que ve només augmentarà el seu pressupost en una partida. Aquesta partida creixerà només un 52% i es dedicarà a pagar els interessos del deute, res més que això. Ho dic per tots aquells que els preocupen les retallades sanitàries.Han de tenir present que l'any que ve serà pitjor. No pas perquè ho digui jo, sino perquè serà el pressupost qui els ho diu.
També podem informar a tots els que volien introduir una nova prestació sanitària , un nou medicament o nova tecnologia mèdica que l'any 2012 no serà el seu any. No pas perquè ho digui jo, sino perquè el pressupost mana.
I tots aquells que diuen que cal apujar els impostos també podem dir-los que el dilema no és més impostos o menys retallades. Aquest és un fals dilema, no hi poden haver més impostos quan el país està trinxat, el món s'ha globalitzat, i som tant solidaris que admetem tenir el tipus marginal més alt i transferim fons a comunitats autònomes on els més rics gaudeixen de tipus marginals més baixos. D'això s'en diu ser solidaris amb els més rics!
Per cert, a Catalunya, entrarem a la part decreixent de la corba?
PS. Si en voleu saber més, sobre la part plana de la corba, podeu consultar aquest editorial de GCS que vam escriure ja fa temps però que manté la seva actualitat.
PS. La perspectiva d'un desaprensiu sobre la crisi econòmica i n'hi ha més d'un.
Aquest estiu s'ha estrenat una nova revista d'economia de la salut "Health Economics Review". Aquesta és una bona notícia i té alhora una novetat destacable, és en accés obert. Un dels primers articles que han sortit ha estat el d'en Zweifel i Shoder que es pregunten en termes agregats si en treiem alguna cosa a canvi de la despesa addicional en assistència sanitària que fem. Dit altrament, si en termes marginals, més recursos han aportat més salut. Llegiu-lo sencer, no hi ha excusa, l'accés és obert. Destaco paràgrafs clau:
From 1960 to 2004 health care expenditure (HCE) of OECD countries increased from 3.8 percent of GDP to 8.9 percent on average. Over the same period, health outcomes measured by average life expectancy at birth improved from 68.4 to 78.5 years. However, this increase has slowed recently. In the United States e.g., it has been 0.19 percent p.a. between 1980 and 2004, down from 0.3 between 1960 and 1980. Since HCE continued to grow at a rate of 7.7 percent p.a. between 1980 and 2004, this has often been interpreted as evidence of decreasing marginal returns ("flat-of-the-curve medicine"]), raising the question of why citizens and governments failed to reallocate resources away from medicine.
Using the standard deviation of life expectancy in 24 OECD countries between 1960 and 2005, a 10 percent increase of health care expenditure isassociated with a decrease of an estimated 0.42 percent. Willingness to pay for such a reduction of uncertainty may well exceed the extra health care expenditure in the United States and Switzerland. This implies that even inthese two countries with very high health care expenditure per capita, flat-of-the-curve medicine need not be wasteful.La seva conclusió seria esperançadora, més recursos per la salut no s'han malbaratat necessàriament. Ara bé la importància de les hipòtesis, les variables utilitzades i la metodologia esdevé fonamental. Si bé es tracta d'un article molt treballat, els propis autors admeten les limitacions que poden tenir les seves conclusions. Jo a més a més, n'hi afegiria una addicional, han pres com a unitat d'observació els països OCDE i una variable controvertida, esperança de vida. Les variacions que hi ha en l'esperança de vida dins un país són moltes (diferències en homes de fins a 2,6 anys, i en dones 3 anys), i en l'esperança de vida activa encara més. I no cal comentar en despesa. Per tant si canvia la unitat d'anàlisi, crec que es podria trobar amb sorpreses majúscules en la conclusió.
PS. Ahir es va anunciar al Parlament que hi ha un país que l'any que ve només augmentarà el seu pressupost en una partida. Aquesta partida creixerà només un 52% i es dedicarà a pagar els interessos del deute, res més que això. Ho dic per tots aquells que els preocupen les retallades sanitàries.Han de tenir present que l'any que ve serà pitjor. No pas perquè ho digui jo, sino perquè serà el pressupost qui els ho diu.
També podem informar a tots els que volien introduir una nova prestació sanitària , un nou medicament o nova tecnologia mèdica que l'any 2012 no serà el seu any. No pas perquè ho digui jo, sino perquè el pressupost mana.
I tots aquells que diuen que cal apujar els impostos també podem dir-los que el dilema no és més impostos o menys retallades. Aquest és un fals dilema, no hi poden haver més impostos quan el país està trinxat, el món s'ha globalitzat, i som tant solidaris que admetem tenir el tipus marginal més alt i transferim fons a comunitats autònomes on els més rics gaudeixen de tipus marginals més baixos. D'això s'en diu ser solidaris amb els més rics!
Per cert, a Catalunya, entrarem a la part decreixent de la corba?
PS. Si en voleu saber més, sobre la part plana de la corba, podeu consultar aquest editorial de GCS que vam escriure ja fa temps però que manté la seva actualitat.
PS. La perspectiva d'un desaprensiu sobre la crisi econòmica i n'hi ha més d'un.
26 de març 2015
The identified person bias
Identified versus Statistical Lives: An Interdisciplinary Perspective
The concept:
The concept:
The identified person bias: A greater inclination to assist (and avoid harming) persons and groups identified as those at high risk of great harm than to assist (and avoid harming) persons and groups who will suffer (or already suffer) similar harm but are not identified (as yet).The issues:
The book, a must read:
- When precisely does the identified person bias arise? And what exactly does it consist in? For example, is it simply a matter of a very human response to the vivid human faces of people with personal stories, in the hospital ward or on TV screens? Is it something that arises only when the risks are known, only under strict uncertainty, or regardless of how much we can specify the risk? Does that bias arise only when few victims are involved?
- What, if anything, might justify giving priority to identified persons at risk?
- What would be the practical implications for law, public health, medicine, and the environment of accepting the priority given to identified persons, or of forsaking it—if we could successfully do so?
13 de novembre 2011
Al país d'Hipòcrates
Si algú està interessat en saber què està passant a la sanitat grega, al WSJ trobarà un article fort, "Health System Reflects Greece's Ills". Hi ha coses que ja sabíem, com el nivell de corrupció i els copagaments als metges en diner negre dins la sanitat pública. Aquesta és una història que ve de lluny però que WSJ sembla descobrir-la ara.
Enmig de la notícia es parlava que la indústria havia negociat amb el govern la mateixa solució que el "dèficit" de tarifa elèctrica, i no havien arribat a un acord, afortunadament(!).
Insisteixo novament, tots aquells que rebutgen l'austeritat com a política del moment poden impulsar situacions com la descrita a WSJ. I tots aquells que han aprovat pressupostos sense cap mesura d'austeritat, amb els diners dels altres, que s'ho facin mirar perquè els esdeveniments van a una velocitat desconeguda.
PS. Kahneman al NYT , lectura d'interès.
PS. Robert Aumann a la contra de LV, lectura obligatòria. Coincideixo plenament amb ell.
PS. Aprofito el cap de setmana per llegir sobre Goldman Sachs i cada capítol em redueix la meva capacitat de sorpresa. Miro les notícies i ja els tenim més aprop, president del BCE i president del govern italià. Encara més aprop hi ha noms que sonen. Compte, seguirem amatents.
PS. Habermas truca a FAZ i fa un article quan veu que les coses es posen magres. El passat dia 5 en va publicar un d'important sobre la feblesa democràtica d'Europa. Els fets recents simplement mostren que no li han fet cas.
PS. Creixent contaminació ambiental, verbal i ideológica en aquest moment. Alguns (pocs) demanen al bisbe que es pronunciï sobre les retallades!. Posats a fer-ho crec que ho haurien de demanar al Papa, que té més autoritat. "Quan una sola malaltia ataca a moltes persones alhora, cal atribuir la causa a allò que és més comú, i que és precisament l'aire que respirem". Hipòcrates dixit p.34. Toca canviar d'aires.
PS. El cost de ser espanyol augmenta cada dia que passa.

Public health care's strained finances have created a large private system, widely used by wealthier Greeks, as well as a shadow system built heavily on bribes—the envelopes of cash known in Greece as fakelaki. Generally, €20 to €50 buys a fast, basic office visit; surgeries can be thousands of euros, according to figures from Transparency International, the anticorruption group, which rates Greece the European Union's most corrupt country.Enmig del text observo:
Instead of money, the drug companies were given government bonds to settle €5.4 billion in unpaid bills from 2007 to 2009. The bonds amounted to nearly 20% less than the full sum, and the firms fear they may see further discounts in the coming debt restructuringFa pocs dies vaig llegir per aquí una cosa similar, enlloc de bons, uns fons voltor es quedarien amb el deute farmacèutic (precisament la mateixa xifra de 5 mil milions, quina casualitat) amb un descompte del 30 a 50%. Una altra casualitat, si s'aplica finalment la quitança al deute grec també representaria un 50% menys per la indústria farmacèutica grega, quina coincidència.
Enmig de la notícia es parlava que la indústria havia negociat amb el govern la mateixa solució que el "dèficit" de tarifa elèctrica, i no havien arribat a un acord, afortunadament(!).
Insisteixo novament, tots aquells que rebutgen l'austeritat com a política del moment poden impulsar situacions com la descrita a WSJ. I tots aquells que han aprovat pressupostos sense cap mesura d'austeritat, amb els diners dels altres, que s'ho facin mirar perquè els esdeveniments van a una velocitat desconeguda.
PS. Kahneman al NYT , lectura d'interès.
We often interact with professionals who exercise their judgment with evident confidence, sometimes priding themselves on the power of their intuition. In a world rife with illusions of validity and skill, can we trust them? How do we distinguish the justified confidence of experts from the sincere overconfidence of professionals who do not know they are out of their depth? We can believe an expert who admits uncertainty but cannot take expressions of high confidence at face value. As I first learned on the obstacle field, people come up with coherent stories and confident predictions even when they know little or nothing. Overconfidence arises because people are often blind to their own blindness.PS. Si enlloc del WSJ voleu un relat més aprofundit consulteu el Lancet . I si voleu consultar l'article clau sobre pagaments informals a Grècia aneu a Health Policy.
PS. Robert Aumann a la contra de LV, lectura obligatòria. Coincideixo plenament amb ell.
PS. Aprofito el cap de setmana per llegir sobre Goldman Sachs i cada capítol em redueix la meva capacitat de sorpresa. Miro les notícies i ja els tenim més aprop, president del BCE i president del govern italià. Encara més aprop hi ha noms que sonen. Compte, seguirem amatents.
PS. Habermas truca a FAZ i fa un article quan veu que les coses es posen magres. El passat dia 5 en va publicar un d'important sobre la feblesa democràtica d'Europa. Els fets recents simplement mostren que no li han fet cas.
PS. Creixent contaminació ambiental, verbal i ideológica en aquest moment. Alguns (pocs) demanen al bisbe que es pronunciï sobre les retallades!. Posats a fer-ho crec que ho haurien de demanar al Papa, que té més autoritat. "Quan una sola malaltia ataca a moltes persones alhora, cal atribuir la causa a allò que és més comú, i que és precisament l'aire que respirem". Hipòcrates dixit p.34. Toca canviar d'aires.
PS. El cost de ser espanyol augmenta cada dia que passa.

Diego Rivera al MOMA
Diego Rivera. Agrarian Leader Zapata. 1931. Fresco, 7' 9 3/4" x 6' 2" (238.1 x 188 cm). The Museum of Modern Art. Abby Aldrich Rockefeller Fund
Diego Rivera. Agrarian Leader Zapata. 1931. Fresco, 7' 9 3/4" x 6' 2" (238.1 x 188 cm). The Museum of Modern Art. Abby Aldrich Rockefeller Fund
08 de novembre 2020
Drug approval and geographic differences
We know that the regulation of medical devices is quite different between US and Europe, and with COVID tests we have experienced such divide. In drugs, one could expect a closer approach to approval. However, this is not the case.
Regulatory agencies may have limited evidence on the clinical benefits and harms of new drugs when deciding whether new therapeutic agents are allowed to enter the market and under which conditions, including whether approval is granted under special regulatory pathways and obligations to address knowledge gaps through postmarketing studies are imposed.
In a matched comparison of marketing applications for cancer drugs of uncertain therapeutic value reviewed by both the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA), we found frequent discordance between the two agencies on regulatory outcomes and the use of special regulatory pathways. Both agencies often granted regular approval, even when the other agency judged there to be substantial uncertainty about drug benefits and risks that needed to be resolved through additional studies in the postmarketing period.
Postmarketing studies imposed by regulators under special approval pathways to address remaining questions of efficacy and safety may not be suited to deliver timely, confirmatory evidence due to shortcomings in study design and delays, raising questions over the suitability of the FDA’s Accelerated Approval and the EMA’s Conditional Marketing Authorization as tools for allowing early market access for cancer drugs while maintaining rigorous regulatory standards.
Hockney
23 d’abril 2020
Behavioral response to the virus
Using Behavioural Science to Help Fight the Coronavirus
Main topics of the paper:
Main topics of the paper:
(1) Evidence on handwashing shows that education and information are not enough. Placing hand sanitisers and colourful signage in central locations (e.g. directly beyond doors, canteen entrances, the middle of entrance halls and lift lobbies) increases use substantially. All organisations and public buildings could adopt this cheap and effective practice.
(2) By contrast, we lack direct evidence on reducing face touching. Articulating new norms of acceptable behaviour (as for sneezing and coughing) and keeping tissues within arm’s reach could help.
(3) Isolation is likely to cause some distress and mental health problems, requiring additional services. Preparedness, through activating social networks, making concrete isolation plans, and becoming familiar with the process, helps. These supports are
important, as some people may try to avoid necessary isolation.
(4) Public-spirited behaviour is most likely when there is clear and frequent communication, strong group identity, and social disapproval for those who don’t comply. This has implications for language, leadership and day-to-day social interaction.
(5) Authorities often overestimate the risk of panic, but undesirable behaviours to watch out for are panic buying of key supplies. Communicating the social unacceptability of both could be part of a collective strategy.
(6) Evidence links crisis communication to behaviour change. As well as speed, honesty and credibility, effective communication involves empathy and promoting useful individual actions and decisions. Using multiple platforms and tailoring message to
subgroups are beneficial too.
(7) Risk perceptions are easily biased. Highlighting single cases or using emotive language will increase bias. Risk is probably best communicated through numbers, with ranges to describe uncertainty, emphasizing that numbers in the middle are more likely. Stating a maximum, e.g. “up to X thousand”, will bias public perception.
03 de gener 2018
Regulatory uncertainty in "home-brew" lab testing
Laboratory-Developed Tests: A Legislative and Regulatory Review
In vitro diagnostics regulation requires continuous adaptation to technologic innovation. Unfortunately, there is a lack of understanding that such a crucial task should be performed efficiently. Europe has waited 23 years for a new regulation!. Anyway, US is under the same trend. Laboratory developed tests were initially regulated 25 years ago and there are still pending issues in the new draft legislation. If you want to know the details, an article in Clinical Chemistry explains the whole issue.

In vitro diagnostics regulation requires continuous adaptation to technologic innovation. Unfortunately, there is a lack of understanding that such a crucial task should be performed efficiently. Europe has waited 23 years for a new regulation!. Anyway, US is under the same trend. Laboratory developed tests were initially regulated 25 years ago and there are still pending issues in the new draft legislation. If you want to know the details, an article in Clinical Chemistry explains the whole issue.
A quarter of a century after the FDA first asserted regulatory authority over LDTs in a draft guidance document, rules and/or guidance regarding LDT oversight have not been implemented. As such, legal questions regarding MDA authority over LDTs and the FDA draft guidance approach have neither been escalated to nor resolved by the judiciary. In addition, many questions central to this debate have not been answered. Are clinical laboratories manufacturers? Should laboratory devices and procedures be regulated similarly? Are there always clear limits between laboratory operations and the practice of laboratory medicine? Any future LDTregulatory or legislative efforts will need to balance and address these concerns if they are to be successful. It is unlikely that interpretation of current statutes and regulations can fully resolve these issues.

Josep Moscardó, Barcelona landscape
02 de juliol 2014
Positive and negative risk cultures
Risk Savvy
While reading The Guardian I find out that Nudge theories could fall from the mainstream.:
His work goes beyond such criticism and it is an additional perspective on how we take decisions and the role of risk and uncertainty.
He considers that health sector is dominated by a negative risk culture, a way of doing that tries to hide errors and in such situations learning is much more difficult. On the other end of the spectrum are "positive error cultures that make error transparent, encorage good errors and learn from bad errors to create a safer environment". This is the case of commercial aviation. From his view, the use of check lists and safety measures should be boosted in many settings to improve efficiency.
Gigerenzer work is a good recommendation for summer reading. Wether he is able to convince you more than Kahneman, it's uncertain right now.
While reading The Guardian I find out that Nudge theories could fall from the mainstream.:
Though nudge-economics remains seductive, what once seemed like a panacea has come to look a bit more like a series of sticking plasters. Earlier this year the nudge unit was removed from direct government control, partly sold to the Nesta innovation charity run by New Labour guru Geoff Mulgan, a move which seemed to suggest the prime minister no longer viewed it as quite so central to his philosophy. That move has coincided with a backlash, or at least a critical analysis, of some of the tenets on which its brand of behavioural economics is based.You already know from this blog I have devoted many posts to it. And I've said many times that its application is still in its beginings. However, if you look at the new book by Gerd Gigerenzer "Risk Savvy", maybe the perspective could be otherwise. He examines Kahneman works and gives a different view. The issue of two systems of the brain, A and B, when taking decisions is under criticism. He defends heuristics that in some sense use both when taking some difficult decisions.
His work goes beyond such criticism and it is an additional perspective on how we take decisions and the role of risk and uncertainty.
He considers that health sector is dominated by a negative risk culture, a way of doing that tries to hide errors and in such situations learning is much more difficult. On the other end of the spectrum are "positive error cultures that make error transparent, encorage good errors and learn from bad errors to create a safer environment". This is the case of commercial aviation. From his view, the use of check lists and safety measures should be boosted in many settings to improve efficiency.
Gigerenzer work is a good recommendation for summer reading. Wether he is able to convince you more than Kahneman, it's uncertain right now.
29 de maig 2020
Healthcare built around you?
Bezonomics
How Amazon Is Changing Our Lives, and What the World's Companies Are Learning from It
Amazon Care
Atul Gawande departure from Haven, the alliance between Amazon, JP Morgan and Berkshire for developing health services for their workers has created uncertainty about what is really Amazon going to do.
Anyway, if you look at the web you can check what is already doing for their employees: Amazon Care. Here you'll find the FAQS. Up to now everybody was thinking about health goods and businesses that Amazon could provide (details in this report). Right now they have started a pilot of health system that may be developed anywhere. A platform business, that starts slowly with and app and a physicians group.
If you want to undestand what Amazon really means for the economy (and for healthcare) than a new book can provide you some answers: Bezonomics.

How Amazon Is Changing Our Lives, and What the World's Companies Are Learning from It
Amazon Care
Atul Gawande departure from Haven, the alliance between Amazon, JP Morgan and Berkshire for developing health services for their workers has created uncertainty about what is really Amazon going to do.
Anyway, if you look at the web you can check what is already doing for their employees: Amazon Care. Here you'll find the FAQS. Up to now everybody was thinking about health goods and businesses that Amazon could provide (details in this report). Right now they have started a pilot of health system that may be developed anywhere. A platform business, that starts slowly with and app and a physicians group.
If you want to undestand what Amazon really means for the economy (and for healthcare) than a new book can provide you some answers: Bezonomics.
The global business world will eventually divide into two camps—those who adopt their own version of Bezonomics, and those who don’t. Alphabet, Facebook, Netflix, Alibaba, JD.com, and Tencent have built huge, powerful businesses based on their ability to collect and analyze data, and keep applying those learnings to make their businesses smarter and their offerings to customers more attractive. In their pursuit of AI-driven technologies such as voice and facial recognition, the Internet of Things, and robotics, they’re creating automated business models that will crush traditional businesses that fail to adapt to this new world. And the emergence of 5G technology, which will replace our current digital networks, will only widen the gap. Experts predict that this next generation of Internet connectivity will be as much as a hundred times faster than today’s web.A must read. In my opinion, what really brings Bezonomics to healthcare is the largest expression of commercialism. In other words, healthcare built around excedent appropriation, not around the patient. If this is so (and Atul Gawande departure is a signal) then we all have to stand up against this model and create value and platforms based on professionalism.
The impact that Bezonomics is having on society is just as profound. Some of the big tech companies are sowing discord with fake news, interfering with elections, and violating personal privacy. As Apple CEO Tim Cook put it: “If you’ve built a chaos factory, you can’t dodge responsibility for the chaos.” The global wealth gap has become so out of kilter that politicians in America and Europe have singled out Amazon and other big tech companies for blame. These wealth-creation machines have become so efficient at creating riches for their top employees and shareholders that they’re likely to engender more public outrage and become easy targets for regulators—perhaps in some cases even be broken up.
11 de març 2018
The rethorical work of modern medicine
Bodies in Flux; Scientific Methods for Negotiating Medical Uncertainty
Evidence and persuasion play a crucial role in everyday task of any physician. That is, knowing the evidence of what works, and persuading that the treatment will succeed in a specific disease.

Evidence and persuasion play a crucial role in everyday task of any physician. That is, knowing the evidence of what works, and persuading that the treatment will succeed in a specific disease.
But how are evidential worlds assembled from bodies in perpetual flux? From where does medicine’s evidential weight hail? What protocols and procedures elevate everyday
biological activities to positions of argumentative authority?
Defining and diagnosing disease is a kind of quixotic empiricism. It requires taking what’s known now and making best guesses about what’s to come. Yet, as physicist and philosopher David Bohm (1981) argues, “all is flux”
After nearly a decade of studying evidential construction in the biomedical backstage, I have identified four specific methods with which medical professionals attune to corporeal flux in cancer care: evidential visualization, assessment, synthesis, and computation.These are the approaches that a new book highlights in detail. In chapter 6 I suggest you read the section "Medical care as phronesis",
Phronesis is one of “the five expressions of care discussed in Book VI of the Ethics” and is a “mode that deals with the contingent and the possible”. Typically, phronesis (defined by Aristotle in the Nicomachean Ethics as “prudence”) is set counter to another rhetorical construct, metis.A book highly recommended for those that want a fresh perspective on evidence based medicine and rethorics.

16 de desembre 2014
Vertical equity in waiting lists
Three years ago I explained that it was good to know that prioritisation was going to start on the waiting lists. It was only the anouncement. Afterwards, it came the uncertainty after a phone call. On March 7th, 2013 the headline post of this blog was: Still waiting after all these months.
Many theoretical efforts have been devoted to improve vertical equity in waiting lists, now it's time to apply them. The moment of truth arrives when somebody has to apply objective criteria, and this raises concerns on the status quo. This is precisely what it comes to my mind when reading this document. I can't find any reference to shared decision-making with patients, taking into account their interests and social preferences. It emphasizes the autonomy of the physicians for waiting lists management, but this is absolutely not enough.
Finally, the document says that budget cuts have to finish. Is this a political or a professional statement?. Everybody should know that budget cuts are related to our critical economic situation, with an unacceptable fiscal deficit. Why is there no reference to this constraint?. Is this a political or a professional option?
Many theoretical efforts have been devoted to improve vertical equity in waiting lists, now it's time to apply them. The moment of truth arrives when somebody has to apply objective criteria, and this raises concerns on the status quo. This is precisely what it comes to my mind when reading this document. I can't find any reference to shared decision-making with patients, taking into account their interests and social preferences. It emphasizes the autonomy of the physicians for waiting lists management, but this is absolutely not enough.
Finally, the document says that budget cuts have to finish. Is this a political or a professional statement?. Everybody should know that budget cuts are related to our critical economic situation, with an unacceptable fiscal deficit. Why is there no reference to this constraint?. Is this a political or a professional option?
29 de setembre 2016
Beyond cost-effectiveness analysis
Departures from Cost-Effectiveness Recommendations: The Impact of Health System Constraints on Priority Setting
Cost-effectiveness may be considered a focal point for health economists. However the trip from theory to implementation raises many doubts. The reductionist perspectives of some health economists consider that politicians are rational in decision making. And this is not the case. I suggest you a look at this article:

Cost-effectiveness may be considered a focal point for health economists. However the trip from theory to implementation raises many doubts. The reductionist perspectives of some health economists consider that politicians are rational in decision making. And this is not the case. I suggest you a look at this article:
The cost-effectiveness model generally used for the evaluation of health technologies—and health care and public health interventions more widely—has become a central tool for public-sector policy makers in many health care systems. It was developed to help decision makers with fixed public resources to compare (1) different interventions for the same health problem and (2) programs in different disease areas. For a particular level of health care resources, the goal is to
choose from among all possible combination of programs the set that maximizes total health benefits produced. The traditional CEA methods presume the existence of only one salient constraint— the public finance budget constraint. Yet all of the evidence suggests that many other constraints impinge on decision makers, at least in the short run.
A fundamental reason for the failure to implement is that CEA assumes a single constraint, in the form of the budget constraint, whereas in reality decision makers may be faced with numerous other constraints. The objective of this article is to develop a typology of constraints that may act as barriers to implementation of cost-effectiveness recommendations. Six categories of constraints are considered: the design of the health system; costs of implementing change; system interactions between interventions; uncertainty in estimates of costs and benefits; weak governance; and political constraints.
There is intelligent life beyond cost-effectiveness...
08 de juliol 2015
Beware of competition in healthcare
Competition among Health Care Providers – Investigating Policy Options in the European Union
Let's imagine an official in European Commission. They are in favour of more competition in health care and asks an expert committee to assess the issue. This is the concrete answer in selected statements from the report:

Let's imagine an official in European Commission. They are in favour of more competition in health care and asks an expert committee to assess the issue. This is the concrete answer in selected statements from the report:
First, and foremost, introducing or increasing competition in the provision of health care services is a delicate policy exercise. The conditions for success and risks for failure need to be carefully assessed. In the right context, introducing competition may help to meet some health system objectives, although it is unlikely to contribute simultaneously and positively to all.Now it is crystal clear. The official has had a precise answer that it is exactly the opposite they were expecting. I've said the same in this blog several times. Take care.
Neither economic theory nor empirical evidence support the conclusion that competition should be promoted in all health services
Neither competition nor strict reliance on government regulation will solve all health system problems. Attempts to avoid or correct market failure can result in government failure and vice versa.
Provider competition can contribute to improving value in health service delivery, but details about where, when and how to introduce competition are critical. Competition in health care provision will not solve all health system problems and may have adverse effects.
Competition is unlikely to achieve improvement in all aspect of health system performance at the same time. It will not solve all the trade-offs policy makers face between different, sometimes conflicting, health system objectives.
Competition can at the same time increase the number of services provided and billed, creating uncertainty in relation to overall health care costs. That is, the introduction of competition may well result in increased costs and add to fiscal pressures. Increased costs may, or may not, be justified by additional health benefits to the population (or some parts of the population).
As competition is an instrument, sound policy evaluation studies are needed to assess and judge its effects. Such empirical studies are currently rare and even absent in some countries.
The introduction of competition has uncertain effects on equity of access to health care, as it is conditional on the effects above and on the heterogeneity of patients. Empirical work has found that the introduction of competition among hospitals, in the UK, produced little or no result in equity terms. This limited evidence does not allow for general presumptions about the effects of competition on equity of access to health care.

19 d’agost 2014
Statistical vs. identifiable lives
Do We Really Value Identified Lives More Highly Than Statistical Lives?
The recent Ebola evacuated case exemplifies the concept created by Shelling a long time ago, the difference of how a society allocates resources according to 2 different rules:
PS. A must read post on GCS blog about the same topic.
PS. Ebolanomics, the economics of ebola at the New Yorker. Nothing new, prizes instead of patents to promote R&D, a good idea with difficult implementation.
PS. How much would you pay for a quality adjusted life year?
The recent Ebola evacuated case exemplifies the concept created by Shelling a long time ago, the difference of how a society allocates resources according to 2 different rules:
In 1968, in a paper about valuing ways to reduce the risk of death, Thomas Schelling1 distinguished between “identified lives” and “statistical lives.” Identified lives are the miners trapped in a mine or the child with a terminal disease—specific people who need help now. Statistical lives are those people, unidentifiable before the fact and often after as well, who will be saved by a new safety regulation, public health program, or environmental standard. Schelling observed that people seem to be willing to pay more to save an identified life: “Let a six-year-old girl with brown hair need thousands of dollars for an operation that will prolong her life until Christmas, and the post office will be swamped with nickels and dimes to save her. But let it be reported that without a sales tax the hospital facilities of Massachusetts will deteriorate and cause a barely perceptible increase in preventable deaths—not many will drop a tear or reach for their checkbooks.Really such a case goes beyond Shelling insight because of uncertainty and unavailability of effective treatment. Bioethics field has argued over what they called "rule of rescue", a different perspective of the same issue. In this respect, NICE statement helps to understand both views:
When there are limited resources for healthcare, applying the ‘rule of rescue’ may mean that other people will not be able to have the care or treatment they need. NICE recognises that when it is making its decisions it should consider the needs of present and future patients of the NHS who are anonymous and who do not necessarily have people to argue their case on their behalf. NICE considers that the principles provided in this document are appropriate to resolve the tension between the needs of an individual patient and the needs of present and future users of the NHS. The Institute has not therefore adopted an additional ‘rule of rescue.The article by Louise B. Rusell reflects precisely the theoretical and practical controversy and ends with this paragraph:
Adjustments and controversies aside, the evidence provided by VSL estimates suggests that people’s willingness to pay for statistical lives may be consistent with their willingness to pay for identified lives. The apparent existence of 2 different decision rules may have been no more than an artifact of the economic method for valuing statistical lives in use at the time the distinction was proposed. Now that economists’ methods more fully reflect “the interests, preferences and attitudes to risk of those who are likely to be affected by the decisions,” their estimates of the value of a statistical life support the idea that there just may be a single rule: Identified and unidentified lives may be equally valuable. This is good news for decision makers who use cost-benefit and cost-effectiveness analysis to inform decisions.The theoretical suggestion sounds good, nowadays the political decision making reality goes in the opposite way, at least close.
PS. A must read post on GCS blog about the same topic.
PS. Ebolanomics, the economics of ebola at the New Yorker. Nothing new, prizes instead of patents to promote R&D, a good idea with difficult implementation.
PS. How much would you pay for a quality adjusted life year?

13 de setembre 2017
How global health stands?
Measuring progress and projecting attainment on the basis of past trends of the health-related Sustainable Development Goals in 188 countries: an analysis from the Global Burden of Disease Study 2016
The Global Burden of Disease (GBD) report shows in an aggregated way how is the world population health. It tries to give an index, and the summary would be:
Let's have alook at the expenditure side:
PS. By the way, there is a ranking. You'll see that Spain has fallen from 7th to 23rd. Forget it. It is still worse but useless. The health variations inside Spain are so huge that the unit of analysis is wrong.

The Global Burden of Disease (GBD) report shows in an aggregated way how is the world population health. It tries to give an index, and the summary would be:
The median health-related SDG index was 56·7 (IQR 31·9–66·8) in 2016 and country-level performance markedly varied, with Singapore (86·8, 95% uncertainty interval 84·6–88·9), Iceland (86·0, 84·1–87·6), and Sweden (85·6, 81·8–87·8) having the highest levels in 2016 and Afghanistan (10·9, 9·6–11·9), the Central African Republic (11·0, 8·8–13·8), and Somalia (11·3, 9·5–13·1) recording the lowest.Sustainable Development Goals (SDG) were set by UN and there are specific indicators for health. However the study takes into account 37 of the 50 indicators. I have explained before some technicalities about the use of DALYs for such studies. And you may know that I am concerned about its use. Today I would add a new concern, it is the projection to 2030 for all these indicators. In my opinions it is a useless effort. Nobody knows, nad using the past to project the future, it is exactly a guarantee of a mistake. However, The Lancet will publish your article.
Let's have alook at the expenditure side:
By comparing performance on the health-related SDG index in 2016 with total health expenditure and DAH (Development Assistace for Health) per capita received from 2010 to 2014,insights might be gleaned regarding the association between overall health funding and performance on the health-related SDG index and whether DAH is being directed toward those countries with the greatest need. Generally, total health expenditure is positively correlated with performance on the health-related SDG index; however, considerable variation exists at the same level of expenditure. For example, among countries with a health-related SDG index of 30 to 70, the association between total health expenditure per capita and performance varied massively, spanning at least a 7 times difference in spending with similar levels of performance on the health-related SDG index.That's a lot of variation, it would require a closer look. And a clear prescription:
For countries that received DAH between 2010–14, some of the most pronounced differences in cumulative DAH per capita received in the 2016 index were in sub-Saharan Africa, with several countries in southern sub-Saharan Africa posting nearly 3 times more cumulative DAH per capita than a number of countries in central and western sub-Saharan Africa. Most notably, some of the poorest performers on the health-related SDG index, such as the Central African Republic, South Sudan, Somalia, and Niger, received relatively little DAH.All in all, GBD is what we have, it has limitations but it allows to understand the situation. It is unnecessary to project the future, in my opinion. We have to work for the improvement of current population health.
PS. By the way, there is a ranking. You'll see that Spain has fallen from 7th to 23rd. Forget it. It is still worse but useless. The health variations inside Spain are so huge that the unit of analysis is wrong.

Subscriure's a:
Missatges (Atom)