
02 d’abril 2020
01 d’abril 2020
Pandemic storytelling
Pandemics, Publics, and Narrative
How people interpret messages to guide action during a pandemic. This is the topic of this book. The effects of storytelling in health communication are crucial and the book starts with the presumed contagion of swine flu by David Cameron.

How people interpret messages to guide action during a pandemic. This is the topic of this book. The effects of storytelling in health communication are crucial and the book starts with the presumed contagion of swine flu by David Cameron.
Our analysis placed engagements with pandemic storytelling across public life in dialogue with the narratives on the enactment of expert advice. This dual approach helped to establish perspectives on how narratives influence publics to take action, or not. We took the view that narrative does not simply mediate pandemic knowledge and advice by helping to structure it intelligibly and meaningfully. We also questioned the idea that narratives persuade in and of themselves in ways that are not very far removed from now discredited notions of linear, hypodermic communications on matters
of health. We adopted the view that media are thoroughly entangled with experience and that pandemic narratives found there help to constitute subjects and the relationships they have with the expert knowledge systems that underpin public health efforts to manage microbial threats
Unlike states of illness, which depend on determinate biomedical diagnosis and the related transformation of identity and relationality, pandemic experience was most often indeterminate due to the infrequency with which influenza infection is diagnosed in a laboratory and the great variation in influenza symptoms between people, between influenza outbreaks, and even over the course of a particular influenza pandemic.
Pandemic narratives are placeholders for rich metaphors of life under threat. The metaphorical properties of contagion and immunity give pandemic narratives biopolitical resonance, connecting as they do: political imperatives to do with the production of life; the self defined and protected against the other; the milieu interieur scene for commune with microbial invaders and friends; the tensions implied in proximity and distance; and the coconstruction of narrative and knowledge.Somebody will have to write a book about current covid-19 pandemic and the title could be: "We are all soldiers against covid". Nothing to add.
31 de març 2020
Unprepared for a pandemic
Unprepared. Global health in a time of emergency
A book that we forgot to read, but it may help (at least for the next time).
A book that we forgot to read, but it may help (at least for the next time).
This book tells the story of how the fragile and still-uncertain machinery of global health security was cobbled together over a two-decade period, beginning in the early 1990s. It is neither a heroic account of visionary planning by enlightened health authorities, nor a sinister story of the securitization of disease by an ever-expansive governmental apparatus. Rather, it is a story of the assemblage of disparate elements— adapted from fields such as civil defense, emergency management, and international public health—by well-meaning experts and officials and of response failures that have typically led, in turn, to reforms that seek to strengthen or refocus the apparatus.9 The analysis centers on the ways that authorities—whether public health officials, national security experts, life scientists, or other privileged observers—conceptualize and act on an encroaching future of disease emergence. This uncertain future can be taken up and made into an object of present intervention according to multiple rationalities: as an object of probabilistic calculation, as a specter that must be avoided through precautionary intervention, or as a potential catastrophe that cannot be evaded but can only be prepared for.10 In the chapters that follow, we see how these various logics come into tension or combine in response to actual and anticipated disease emergencies.And the key message
The widely acknowledged failure of global health security to adequately manage the Ebola outbreak led to multiple inquiries, commission reports, and recommendations for reform, but it did not put in question the strategic logic underlying the framework. Rather, reformers raised the question of how to better meet the demand for preparedness in time for the next global health emergency. As an internal World Health Organization (WHO) report warned, the frequency and magnitude of such events was increasing but “the world is not adequately prepared to respond to the full range of emergencies with public health implications”—whether disease outbreaks, natural disasters or violent conflict. The report concluded that WHO’s response to Ebola and other recent emergencies “lacked the speed, coordination, clear lines of decision making and dedicated funding to optimize implementation, reduce suffering and save lives.” Given the scale and complexity of anticipated future emergencies, it advised, “WHO must substantially strengthen and modernize its emergency management capacity.”So what? We have to confront right now the emergency and WHO reform is still pending...
30 de març 2020
To test or not to test (for coronavirus) (3)
Current situation on test results

Covid-19 Incidence: 212 per 100.000 inhabitants
Spreading rate: 0,6
This is good news!
29 de març 2020
Psychology of pandemics
The Psychology of Pandemics: Preparing for the Next Global Outbreak of Infectious Disease

The patterns of psychological reactions to pandemics are complex. Whereas some people are resilient to stress, other individuals become highly distressed when confronted with threatening events such as pandemic infection. Thus, people vary widely in their reactions to threatened or actual pandemics. Some react with indifference or resignation while others become highly fearful or anxious, and some develop emotional disorders such as PTSD. Some people recover from these emotional problems once the pandemic threat passes, while other people have enduring emotional reactions. Social disruptive behaviors such as rioting can also occur under particular circumstances, although prosocial behaviors appear to be more common during times of pandemic. Immune reactions may explain some of the emotional responses in infected people but these fail to account for widespread fear and social disruption in people who have not yet been infected. To better understand the reasons behind these diverse psychological reactions it is important to understand their motivational roots and vulnerability factors.This book is devoted precisely to this issue, to understand psychological reactions and its roots.
28 de març 2020
The new science of contagion
In chapter 2 of this book, Adam Kucharski explains the details about R, the crucial parameter in any epidemic. Right now it seems that we are at 2,3 and waiting to decrease below 2.
R is a more intuitive – and general – way to think about contagion. It simply asks: how many people would we expect a case to pass the infection on to? As we shall see in later chapters, it’s an idea that we can apply to a wide range of outbreaks, from gun violence to online memes.PS. The statistics of contagion
R is particularly useful because it tells us whether to expect a large outbreak or not. If R is below one, each infectious person will on average generate less than one additional infection. We’d therefore expect the number of cases to decline over time. However, if R is above one, the level of infection will rise on average, creating the potential for a large epidemic.
Some diseases have a relatively low R. For pandemic flu, R is generally around 1–2, which is about the same as Ebola during the early stages of the 2013–16 West Africa epidemic. On average, each Ebola case passed the virus onto a couple of other people. Other infections can spread more easily. The sars virus, which caused outbreaks in Asia in early 2003, had an R of 2–3.
R therefore depends on four factors: the duration of time a person is infectious; the average number of opportunities they have to spread the infection each day they’re infectious; the probability an opportunity results in transmission; and the average susceptibility of the population. I like to call these the ‘DOTS’ for short. Joining them together gives us the value of the reproduction number:
R = Duration × Opportunities × Transmission probability × Susceptibility

27 de març 2020
Policymakers neglecting science in coronavirus times
Experts’ request to the Spanish Government: move Spain towards complete lockdown
Scientific community in The Lancet:

Scientific community in The Lancet:
We urge the Spanish Government to implement, as swiftly as possible, more drastic measures to minimize the impact of the pandemic on the Spanish population.Policymakers:
The answer is: "We are all soldiers against the virus"!!!
as if the covid-19 was a war...
as if the covid-19 was a war...
This is exactly the level of cinism while people are dying from covid-19.

26 de març 2020
Smart testing in coronavirus pandemic
We need smart coronavirus testing, not just more testing
Key messages by Mostashari and Emanuel:
PS. An epidemic calculator
PS. Current situation of the pandemic in our country.
Key messages by Mostashari and Emanuel:
The first two questions, which will be key to guiding policymakers on whether the extreme measures taken to suppress the outbreak are working, are these: Is the Covid-19 outbreak in a city or state getting better or worse? And how fast?
To know if Covid-19 is getting better or worse, we need to know how the percentage of positive cases — not the number — changes day by day, accounting for delays in testing and reporting and how the percentages change in response to public health measures such as sheltering-in-place or suppression. This will tell us how effective these measures are in curtailing the spread of SARS-CoV-2 and thus whether when social restrictions could be relaxed or additional policies might need to be implemented.
The other two questions that need answers are essential for guiding doctors in their medical decision making: Who is getting Covid-19? And what are their outcomes?
First, as a condition of receiving approval and test kits, laboratories should be required to submit basic information like age, county of residence, and testing site on every person tested — not just the positives.
Second, we need a sero survey of multiple communities. Such studies test blood samples from randomly chosen individuals in a defined population. This is the way to assess the real percentage of people in a community who test positive for recent coronavirus infection. This gives a picture that is wider than just the individuals who are bringing themselves in for testing. Right now we simply have no idea how many Americans are infected with the coronavirus. This will be a key input to models trying to predict when herd immunity can begin to blunt the outbreak.
PS. An epidemic calculator
PS. Current situation of the pandemic in our country.
25 de març 2020
On rationing (ventilators) (2)
Fair Allocation of Scarce Medical Resources in the Time of Covid-19
The four fundamental values for allocating resources, according Ezequiel Emanuel and colleagues are those included in this article:


The four fundamental values for allocating resources, according Ezequiel Emanuel and colleagues are those included in this article:
Maximizing the benefits produced by scarce resources, treating people equally, promoting and rewarding instrumental value, and giving priority to the worst off. Consensus exists that an individual person’s wealth should not determine who lives or dies.And,
Maximization of benefits can be understood as saving the most individual lives or as saving the most life-years by giving priority to patients likely to survive longest after treatment. Treating people equally could be attempted by random selection, such as a lottery, or by a first-come, first-served allocation. Instrumental value could be promoted by giving priority to those who can save others, or rewarded by giving priority to those who have saved others in the past. And priority to the worst off could be understood as giving priority either to the sickest or to younger people who will have lived the shortest lives if they die untreated.
The proposals for allocation discussed above also recognize that all these ethical values and ways to operationalize them are compelling. No single value is sufficient alone to determine which patients should receive scarce resources.24-33 Hence, fair allocation requires a multivalue ethical framework that can be adapted, depending on the resource and context in question.Here you'll find some reflections on how to put this into practice.
Eating in pandemic times
24 de març 2020
Designing a market for lab tests in a pandemic
Alvin Roth in his book sheds light on the field known as Market design. Given a set of agents, market design seeks to identify the game rules that might be implemented and that would produce the desired behaviors in the players. In some markets, prices may be used to induce the desired outcomes—these markets are the study of auction theory. In other markets, prices may not be used—these markets are the study of matching theory.
Until recently, economists often passed quickly over matching and focused primarily on commodity markets, in which prices alone determine who gets what. In a commodity market, you decide what you want, and if you can afford it, you get it.The price does all the work, bringing the two of you together at the price at which supply equals demand.The first question is, can we consider lab tests for a pandemic a commodity?. My impression is that once a virus pandemic has appeared, we need the sequencing for the genome of the virus and after that, several suppliers may offer different options with a high level of uncertainty. Buyers are blind about the options for testing. Suppliers don't know about the extent of the outbreak and the need of tests. The market is rising. In such situations the criteria should be to allocate most of the production to the place where the outbreak has started, in order to prevent contagion. Price may distort this allocation because other countries and buyers may strategically move first to achieve strategic reserves.
Alvin Roth says:
The first task of a successful marketplace is bringing together many participants who want to transact, so they can seek out the best transactions. Having a lot of participants makes a market thick.
Congestion is a problem that marketplaces can face once they’ve achieved thickness. It’s the economic equivalent of a traffic jam, a curse of success. The range of options in a thick market can be overwhelming, and it may take time to evaluate a potential deal, or to consummate it. Marketplaces can help organize potential transactions so that they can be evaluated fast enough that if particular deals fall through, other opportunities will still be available. In commodity markets, price does this well, since a single offer can be made to the entire market (“Anyone can buy a pint of my raspberries for $5.50”), but in matching markets, each transaction may have to be considered separately.
Decisions that depend on what others are doing are called strategic decisions and are the concern of the branch of economics called game theory. Strategic decision making plays a big role in determining who does well or badly in many selection processes. Often when we game theorists study a matching process, we learn how participants “game the system.” Well-designed matching processes try to take into account the fact that participants are making strategic decisions.
When a market doesn’t deal effectively with congestion and participants may not be able to find the transactions they want, it might not be safe for them to wait for the marketplace to open if some opportunities are available earlier. Even when going early isn’t an option, the marketplace might force participants to engage in risky gambles.The range of tests may be overwhelming, as it is right now with coronavirus. How can we manage such congestion?
There is a chapter in the Handbook of Market Design by Paul Klemperer about The Product-Mix Auction: A New Auction Design for Differentiated Goods. I've read what he proposes and I think that fits quite well with the market for lab tests in a pandemic. Of course, additional details are needed. The research question is:
How should goods that both seller(s) and buyers view as imperfect substitutes be sold, especially when multi-round auctions are impractical?
My design is straightforward in concept—each bidder can make one or more bids, and each bid contains a set of mutually exclusive offers. Each offer specifies a price (or, in the Bank of England's auction, an interest rate) for a quantity of a specific "variety." The auctioneer looks at all the bids and then selects a price for each "variety." From each bid offered by each bidder, the auctioneer accepts (only) the offer that gives the bidder the greatest surplus at the selected prices, or no offer if all the offers would give the bidder negative surplus. All accepted offers for a variety pay the same (uniform) price for that variety.
The idea is that the menu of mutually exclusive sets of offers allows each bidder to approximate a demand function, so bidders can, in effect, decide how much of each variety to buy after seeing the prices chosen. Meanwhile, the auctioneer can look at demand before choosing the prices; allowing it to choose the prices ex post creates no problem here, because it allocates each bidder precisely what that bidder would have chosen for itself given those prices. Importantly, offers for each variety provide a competitive discipline on the offers for the other varieties, because they are all being auctioned simultaneously.
Compare this with the "standard" approach of running a separate auction for each different "variety." In this case, outcomes are erratic and inefficient, because the auctioneer has to choose how much of each variety to offer before learning bidders' preferences, and bidders have to guess how much to bid for in each auction without knowing what the price differences between varieties will turn out to be; the wrong bidders may win, and those who do win may be inefficiently allocated across varieties. Furthermore, each individual auction is much more sensitive to market power, to manipulation, and to informational asymmetries than if all offers compete directly with each other in a single auction. The auctioneer's revenues are correspondingly generally lower. All these problems also reduce the auctions' value as a source of information. They may also reduce participation, which can create "second-round" feedback effects further magnifying the problems.
The rules of the auction are as follows:
1. Each bidder can make any number of bids. Each bid specifies a single quantity and an offer of a per-unit price for each variety. The offers in each bid are mutually exclusive.
2. The auctioneer looks at all the bids and chooses a minimum "cut-off" price for each variety
3. The auctioneer accepts all offers that exceed the minimum price for the corresponding variety, except that it accepts at most one offer from each bid. If both price offers in any bid exceed the minimum price for the corresponding variety, the auctioneer accepts the offer that maximizes the bidder s surplus, as measured by the offer's distance above the minimum price.
4. All accepted offers pay the minimum price for the corresponding variety—that is, there is "uniform pricing" for each variety
It is easy to include additional potential sellers (i.e., additional lenders of funds, in our example). Simply add their maximum supply to the total that the auctioneer sells, but allow them to participate in the auction as usual. If a potential seller wins nothing in the auction, the auctioneer has sold the sellers supply for it. If a potential seller wins its total supply back, there is no change in its positionMy impression is that lab tests in a pandemic require a market design, current allocation methods are relying in a free market that doesn't allows to create value where it it most needed.
Just a final words by Alvin Roth:
Because economics touches on just about everything, economists have an opportunity to learn something from just about everyone, and I’ve met and worked with some remarkable people in each of the markets I’ve helped design.
Market design is giving new scope to the ancient profession of matchmaking. Consider this book a tour of the matching and market making happening around us. I hope it will give you a new way to see the world and to understand who gets what—and why.

23 de març 2020
The market for corovanirus tests
The delays in coronavirus testing can be explained by shortage of stocks from the supply side, mismatchs between supply and demand and from incomplete information about the current offer of tests in the market. Somebody should analyse this in detail and give some explanations. Why there is no international body to coordinate such decisions?. Can the market provide an equilibrium and give the right answer to the pandemic testing?.
It is quite surprising that there are so many companies providing such tests. Have a look at this site FINDDX, you'll see many options, from molecular diagnostics to inmunoassays. Unless somebody can assess current production capacity and available stock, current shortages may be a false signal of mismatch.
Up to now everybody has been talking about PCR test, but you may get right now antibody detection IgG IgM and this could add valuable information. Inmunoassay tests would help to understand those who are already inmunized, though with less precision. If so, we could reduce current social distancing prescriptions after a window period. If those that show positive IgG can avoid lockdown, then this could help a lot.
PS. If you want to know how many tests have been performed up to now, check this website.
PS. Just one minor issue. Spain says that has made 30.000 tests. Right now we already have 33.089 confirmed cases !. Data and statistics from Spain are a complete disaster. It is not possible a positive result in more than 100% tests!
It is quite surprising that there are so many companies providing such tests. Have a look at this site FINDDX, you'll see many options, from molecular diagnostics to inmunoassays. Unless somebody can assess current production capacity and available stock, current shortages may be a false signal of mismatch.
Up to now everybody has been talking about PCR test, but you may get right now antibody detection IgG IgM and this could add valuable information. Inmunoassay tests would help to understand those who are already inmunized, though with less precision. If so, we could reduce current social distancing prescriptions after a window period. If those that show positive IgG can avoid lockdown, then this could help a lot.
PS. If you want to know how many tests have been performed up to now, check this website.
PS. Just one minor issue. Spain says that has made 30.000 tests. Right now we already have 33.089 confirmed cases !. Data and statistics from Spain are a complete disaster. It is not possible a positive result in more than 100% tests!
22 de març 2020
On rationing (ventilators)
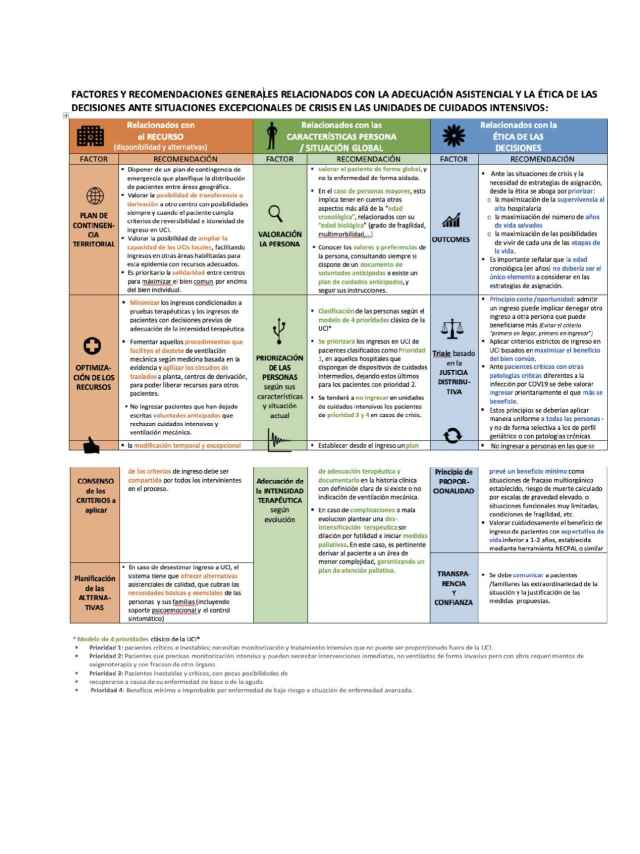
Recomendaciones éticas para tomar decisiones en la situación excepcional de crisis por pandemia Covid-19 en las UCI
These are tough times for mankind. We are social animals and current instructions/recommendations are focused to behave exactly the opposite. Once the coronavirus hits someone, the result may be being hospitalised and one may need intensive care and mechanical ventilation. And if supply is not enough for the demand of ventilators, then starts the most difficult question: who gets the ventilator?. A professional answer is needed. Fortunately the scientific society Sociedad Española de Medicina Intensiva, Crítica y Unidades Coronarias has released a document that helps to provide specific recommendations in such situation.
This is exactly what we can expect from a modern society. Professional decisions need guidance and consensus. There is no role for politicians in this issue and in this moment, scientific societies have to coordinate such efforts. Therefore my congratulations for their recommendations.
Basically, the document highlights the criteria of maximizing capability of benefit, and in the current situation and in intensive care, this has to be applied in a general way, for covid-19 and non covid-19 disease requiring such services. And these criteria should be applied in an uniform way.
In this blog I've been supporting the role of professionalism in taking tough decisions. Today I've to say that these is a good example of rationing to keep in mind.
PS. If projects like this one succeed, then tough decisions could be avoided. Great initiative.
These are tough times for mankind. We are social animals and current instructions/recommendations are focused to behave exactly the opposite. Once the coronavirus hits someone, the result may be being hospitalised and one may need intensive care and mechanical ventilation. And if supply is not enough for the demand of ventilators, then starts the most difficult question: who gets the ventilator?. A professional answer is needed. Fortunately the scientific society Sociedad Española de Medicina Intensiva, Crítica y Unidades Coronarias has released a document that helps to provide specific recommendations in such situation.
This is exactly what we can expect from a modern society. Professional decisions need guidance and consensus. There is no role for politicians in this issue and in this moment, scientific societies have to coordinate such efforts. Therefore my congratulations for their recommendations.
Basically, the document highlights the criteria of maximizing capability of benefit, and in the current situation and in intensive care, this has to be applied in a general way, for covid-19 and non covid-19 disease requiring such services. And these criteria should be applied in an uniform way.
In this blog I've been supporting the role of professionalism in taking tough decisions. Today I've to say that these is a good example of rationing to keep in mind.
PS. If projects like this one succeed, then tough decisions could be avoided. Great initiative.
21 de març 2020
Social distancing in times of pandemics
These are the values in normal conditions:

Huge differences across countries!
Nowadays, during pandemics, social distancing means confinement.
20 de març 2020
Economics of pandemics
There is a new free ebook available on the economics of current pandemics that was finished on March 5h. These are the contents:
Introduction: Richard Baldwin and Beatrice Weder di Mauro
1 Macroeconomics of the fluFrom Joachim Voth chapter:
Beatrice Weder di Mauro
2 Tackling the fallout from COVID-19
Laurence Boone
3 The economic impact of COVID-19
Warwick McKibbin and Roshen Fernando
4 Novel coronavirus hurts the Middle East and North Africa through many channels
Rabah Arezki and Ha Nguyen
5 Thinking ahead about the trade impact of COVID-19
Richard Baldwin and Eiichi Tomiura
6 Finance in the times of coronavirus
Thorsten Beck
7 Contagion: Bank runs and COVID-19
Stephen G. Cecchetti and Kermit L. Schoenholtz
8 Real and financial lenses to assess the economic consequences of COVID-19
Catherine L. Mann
9 As coronavirus spreads, can the EU afford to close its borders?
Raffaella Meninno and Guntram Wolff
10 Trade and travel in the time of epidemics
Joachim Voth
11 On plague in a time of Ebola
Cormac O Grada
12 Coronavirus monetary policy
John H. Cochrane
13 The economic effects of a pandemic
Simon Wren-Lewis
14 The good thing about coronavirus
Charles Wyplosz
First, is a massive restriction of mobility desirable? And second, is it feasible at all? An economically rational answer to the first question should begin with the value of a human life. With all the reservations that one can have against such calculations from a philosophical point of view, cost-benefit considerations without numbers for the value of a human life are not feasible. However, estimates regularly show an enormous range; the average is around US$10 million per person (Viscusi and Masterman 2017). This means that even before the epidemic has peaked, COVID-19 caused an immediate cost of $26 billion in deaths. If the epidemic ends with a maximum of 10,000 deaths (four times the current value), the value of life destroyed would be approximately $100 billion.Up to now,this is the only chapter I've read from these promising book.
The costs must be compared with the enormous gains in economic performance that the free exchange of goods and people has made possible. In China alone, hundreds of millions of people have escaped deepest poverty during the past 20 years. In 1980, more than half of the Chinese population lived on less than $2 a day; in 1998, it was less than a quarter (Sala-i-Martin 2006). Around the world, people have escaped the poverty trap wherever the free movement of goods and people has become possible. And richer regions also benefit massively, often in surprising ways.

Subscriure's a:
Missatges (Atom)