The Ethics of Health Care Rationing: An Introduction
El llibre "The Ethics of Health Care Rationing: An Introduction", escrit per Greg Bognar i Iwao Hirose, és una introducció clara i oportuna al tema universal i inevitable del racionament de l'atenció sanitària. El racionament es produeix tant en països pobres com en els rics, i en sistemes finançats públicament com en els privats. La segona edició del llibre, publicada el 2022, inclou capítols nous sobre la discriminació per discapacitat i edat, i sobre el preu dels fàrmacs i teràpies mèdiques.
Els autors, Greg Bognar (professor sènior a la Universitat d'Estocolm) i Iwao Hirose (catedràtic d'Investigació del Canadà a la Universitat McGill), argumenten que el racionament sanitari no només és inevitable i omnipresent, sinó que també és desitjable, ja que permet l'assignació de recursos d'una manera moralment defensable. Per tal que el racionament sigui ètic, ha de basar-se en principis morals sòlids.
Estructura i Temes Clau del Llibre
El llibre examina les controvèrsies ètiques mitjançant exemples dels Estats Units, el Regne Unit i altres països. Els temes centrals abordats són:
- Quins principis distributius haurien de guiar el racionament sanitari?
- Quina relació hi ha entre l'ètica i la rendibilitat (cost-effectiveness) en l'atenció sanitària?
- Com s'hauria d'abordar la controvèrsia sobre la discriminació per discapacitat i edat?
- Com s'han de tractar les polèmiques entorn del racionament i el preu dels fàrmacs?
- S'ha de fer responsables els pacients de la seva salut?
- Com es relaciona el debat sobre la responsabilitat amb l'estatus socioeconòmic i la desigualtat social?
Els autors destaquen dos principis morals bàsics per al racionament sanitari: la maximització dels beneficis derivats de l'ús dels recursos i la justícia (fairness) en la distribució d'aquests beneficis. A continuació, es resumeixen detalladament els capítols:
Introducció i Fonaments (Capítols 1 i 2)
Capítol 1: Ètica i atenció sanitària
El racionament es defineix com l'assignació controlada de recursos o béns escassos, cosa que implica limitar la seva disponibilitat. El racionament sanitari és inevitable a causa de l'escassetat dels recursos. Aquesta escassetat sorgeix de l'avanç tecnològic (que augmenta la despesa), l'ús excessiu de recursos (com els antibiòtics), i les dificultats d'accés que creen desigualtats.
El capítol utilitza l'exemple dels programes de vacunació per il·lustrar que la majoria de la gent creu que tant la maximització dels beneficis com la justícia (equitat) són consideracions morals rellevants. El racionament es manifesta en la priorització d'intervencions, serveis o fàrmacs, i només ocasionalment implica la selecció de pacients concrets (racionament a la capçalera del llit). Els autors introdueixen els conceptes d'ètica (conceptes deòntics) i conseqüencialisme (conceptes axiològics), essent el conseqüencialisme la visió que la bondat o maldat de les conseqüències determinen la correcció d'un acte.
Capítol 2: El valor de la salut
Per maximitzar els beneficis, cal poder comparar l'assignació de recursos. Com que la salut no és una quantitat mesurable directament, s'ha de mesurar el valor de la salut a través del seu impacte en el benestar o la qualitat de vida (quality of life).
- Mesures de la Qualitat de Vida Relacionada amb la Salut (HRQoL): Els autors examinen mètodes per mesurar l'HRQoL, com l'EQ-5D, que descriu estats de salut mitjançant cinc dimensions.
- Mètodes d'Avaluació: Es descriuen el mètode d'escala de qualificació (rating scale), el mètode de risc estàndard (standard gamble) i el mètode d'intercanvi de temps (time trade-off). Els dos últims s'utilitzen per crear una escala d'interval que permet comparar magnituds de millora.
- QALYs i DALYs: Les avaluacions de l'estat de salut es combinen amb la durada de la vida per crear mesures ajustades a la qualitat, com els Anys de Vida Ajustats per Qualitat (QALY) i els Anys de Vida Ajustats per Discapacitat (DALY).
- QALY: Representa un any de vida en salut plena (valor 1).
- DALY: Mesura la càrrega de malaltia com la diferència entre la salut real i la ideal (valor 0 = salut plena, 1 = mort).
- Problema de qui preguntar: Es qüestiona si s'han d'utilitzar avaluacions de la població general, professionals sanitaris o pacients. Els pacients amb discapacitat sovint s'adapten a la seva condició, valorant-la menys negativament que la població general, la qual cosa pot generar una paradoxa en la priorització.
L'Anàlisi Cost-efectivitat (Capítols 3, 4 i 5)
Capítol 3: Ètica i anàlisi de cost-efectivitat (CEA)
L'Anàlisi cost-efectivitat (Cost-Effectiveness Analysis, CEA) és l'eina principal per avaluar els beneficis per a la salut tenint en compte els costos. Es basa en la ràtio entre el cost i la unitat de benefici (normalment QALYs o DALYs).
- Aplicació: La CEA s'utilitza per crear una llista de prioritats i establir un llindar de rendibilitat.
- Controvèrsia: Els autors defensen la CEA, argumentant que no posa un valor monetari a les vides, sinó que compara el valor de les intervencions.
- Exemples d'ús: Es descriuen casos reals com el Pla de Salut d'Oregon (EUA), que intentava utilitzar la CEA per ampliar la cobertura de Medicaid, la PHARMAC a Nova Zelanda, i el NICE al Regne Unit.
- Ponderació per Equitat (Equity Weighting): Per abordar els problemes de justícia distributiva, es proposa assignar més pes moral als beneficis que recauen en els més desafavorits. Aquest enfocament es basa en el prioritarianisme.
- Descompte (Discounting): Es discuteix la pràctica de descomptar (reduir el valor) els costos i beneficis futurs en els càlculs de CEA. L'abandonament del descompte de DALYs per part del projecte Global Burden of Disease s'esmenta com un cas on els arguments filosòfics van influir en la pràctica.
Capítol 4: Discriminació per discapacitat
S'aborda l'Objecció de Discriminació per Discapacitat, que al·lega que la CEA desavantatja injustament les persones amb discapacitat o malalties cròniques.
- Refutació de l'objecció: L'objecció sovint confon el valor de les persones (que és igual per a tothom) amb la qualitat de la seva vida (que pot ser menor a causa de la discapacitat). A més, la CEA normalment classifica intervencions, no pacients. La CEA tendeix a afavorir el tractament dels que tenen una qualitat de vida baixa, ja que poden aconseguir una millora major.
- Limitació de la capacitat de benefici: Es reconeix que els pacients amb discapacitat permanent poden tenir una capacitat de benefici limitada, donant lloc a una ràtio cost/QALY menys favorable per a certes intervencions que coexisteixen amb la seva discapacitat.
- Problema de Desavantatge: El veritable problema moral no és la discriminació, sinó la possibilitat que grups específics (per exemple, amb una malaltia rara) quedin desavantatjats si la seva única intervenció possible no és rendible. Es suggereix que aquest desavantatge s'ha d'abordar mitjançant la ponderació per equitat.
Capítol 5: La qüestió de l'edat
Aquest capítol examina si l'edat hauria de ser un criteri per al racionament.
- Argument del "Fair Innings" (Oportunitat Justa): Aquesta visió sosté que la prioritat s'ha de donar als joves per garantir que tothom tingui l'oportunitat de viure una vida completa ("fair innings"), establint un llindar d'edat (per exemple, 70 anys).
- Edatisme Utilitari: La CEA sovint afavoreix els joves de manera natural, ja que un tractament per a un jove genera més QALYs (benefici a llarg termini) que el mateix tractament per a una persona gran. Això s'anomena edatisme utilitari.
- Ponderació per Edat (Age-Weighting): Es proposa modificar la CEA amb una ponderació per edat per reflectir la rellevància moral de l'edat.
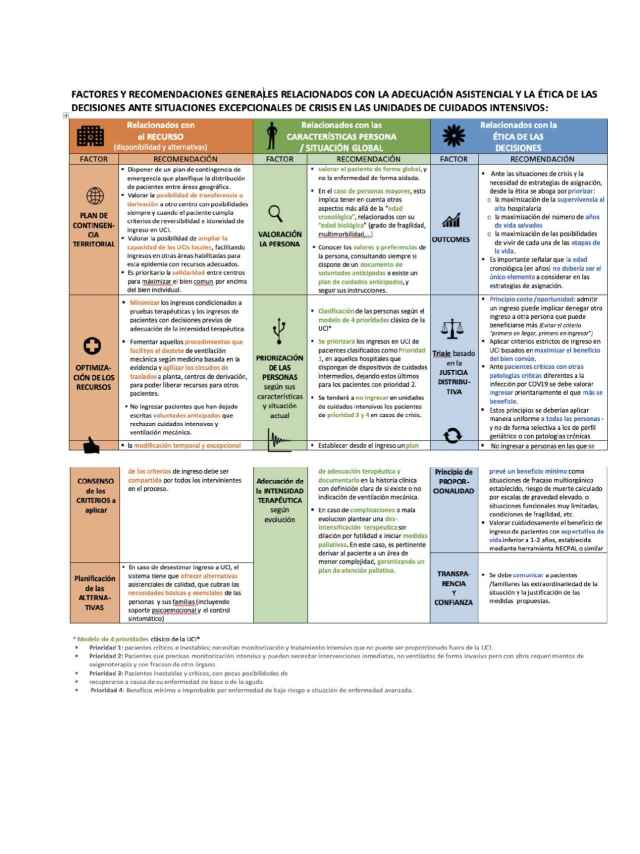
- Racionament a la Capçalera del Llit (Bedside Rationing): L'edat esdevé crucial en situacions d'escassetat extrema, com durant la pandèmia de COVID-19. Alguns sistemes van utilitzar l'edat com a criteri (o "trencador d'empat") per a l'admissió a l'UCI.
- DALYs i Ponderació per Edat: Les primeres versions dels DALYs aplicades al projecte Global Burden of Disease utilitzaven una funció de ponderació per edat amb forma de gep (donant el màxim pes entre els 20 i 30 anys). Aquesta pràctica va ser abandonada el 2010 a causa de la controvèrsia.
Problemes d'Agregació i Distribució (Capítols 6 i 7)
Capítol 6: L'agregació dels beneficis per a la salut
El principi de maximització dels beneficis es basa en la Tesi d'Agregació, que permet sumar els beneficis individuals (QALYs) per a l'avaluació moral.
- Problema de l'Agregació: Sorgeix quan petits beneficis per a un gran nombre de persones podrien superar grans beneficis per a un petit nombre. L'exemple d'Oregon de classificar l'obtenció de fundes dentals (tooth capping) per sobre de l'apendicectomia il·lustra aquesta possible implicació contraintuïtiva de la CEA.
- Problema del Nombre: Si es rebutja la Tesi d'Agregació (com en el principi de comparació per parelles), es genera el problema del nombre: hauríem de ser indiferents entre salvar moltes vides i salvar-ne una, ja que la pèrdua individual és la mateixa.
- Prioritarianisme: Es presenta com una solució que permet l'agregació (evitant el problema del nombre) alhora que dóna més pes als beneficis que recauen en els més desafavorits. Així, es mitiga la implicació contraintuïtiva de la CEA.
- Loteria Ponderada: S'examina com un mètode per assignar una "oportunitat justa" (fair chance) als individus, sent sensible al nombre sense sumar els beneficis.
Capítol 7: Responsabilitat per la salut
Es qüestiona si la responsabilitat individual per la salut (per exemple, fumar o obesitat) hauria d'afectar la prioritat en l'assignació de recursos sanitaris.
- Igualitarisme de la Sort (Luck Egalitarianism): Aquesta filosofia sosté que les desigualtats degudes a la sort bruta (fora del control individual) s'han de compensar, però les degudes a la sort d'opció (resultat de decisions intencionals) no generen preocupacions de justícia. Segons aquesta visió, un fumador amb malaltia cardíaca (sort d'opció) hauria de tenir menys prioritat que un no fumador amb la mateixa malaltia (sort bruta).
- Objecció d'Abandonament (Abandonment Objection): L'igualitarisme de la sort es considera massa dur (harsh) perquè implica que la societat no té l'obligació de justícia d'ajudar aquells responsables de la seva mala sort, fins i tot si es disposa de recursos.
- Alternatives: Es proposa que la responsabilitat s'abordi fora del sistema sanitari (per exemple, mitjançant impostos elevats sobre el tabac o l'alcohol), de manera que al punt de tractament tots els pacients siguin tractats per igual.
- Gradient Social de la Salut: Es discuteix la forta correlació entre l'estatus socioeconòmic (ingressos, educació) i els resultats de salut, suggerint que la mala salut no és una "elecció" lliure, sinó que està determinada per factors socials. Això desafia la idea d'una responsabilitat individual clara i limita el paper de la responsabilitat en el racionament sanitari.
El Preu dels Fàrmacs (Capítol 8)
Capítol 8: El preu dels fàrmacs
Aquest capítol, nou en la segona edició, examina el paper dels costos dels fàrmacs en el racionament i en la sostenibilitat del sistema sanitari.
- La CEA com a eina de control de preus: La CEA, mitjançant l'establiment d'un llindar de rendibilitat, pot obligar les empreses farmacèutiques a oferir descomptes (com el Patient Access Scheme del NICE al Regne Unit) per mantenir el preu d'un fàrmac dins del que la societat considera raonable.
- Contrast Japó vs. Regne Unit:
- Japó: El govern estableix els preus mitjançant el mètode de càlcul de costos, independentment dels beneficis per a la salut, la qual cosa incentiva els fabricants a inflar els costos i pot conduir a preus extremadament alts per a fàrmacs innovadors sense comparador.
- Regne Unit (NICE): Utilitza la CEA per avaluar la rendibilitat. La possibilitat de no ser recomanat pel NICE actua com una amenaça creïble que indueix els fabricants a negociar preus més baixos.
- Fàrmacs "Massa Barats": Es discuteix la paradoxa que preus massa baixos redueixen els marges de benefici de la indústria, cosa que pot conduir a l'escassetat mundial d'antibiòtics o a la manca d'incentius per a la R+D de fàrmacs orfes (per a malalties rares).
Conclusió
Els autors reiteren que el racionament és desitjable, ja que garanteix una assignació de recursos justa, transparent i rendible, i evita que les decisions difícils recaiguin exclusivament en els metges a la capçalera del llit. El llibre conclou que, tot i la complexitat dels principis de justícia, la rendibilitat i la justícia són ideals ètics essencials per guiar el racionament sanitari.
El llibre no pren posició sobre la millor organització o finançament del sistema sanitari, ja que els arguments presentats són independents de si el sistema és públic o privat. A més, cap argument en el llibre suggereix que l'única manera de fer front a l'escassetat sigui reduir la despesa sanitària.
PS. Tasa de fertilitat