
07 d’abril 2014
04 d’abril 2014
A primer on health economics and policy
Social values in health and social care
In just 38 pages Tony Culyer explains the basics of health policy. It is not a review, these are a collection of key insights that basically come from his book. This is the outline:
.
In just 38 pages Tony Culyer explains the basics of health policy. It is not a review, these are a collection of key insights that basically come from his book. This is the outline:
- Introduction
- Liberalism versus libertarianism
- The market versus the state
- Public versus private insurance
- Equity versus equality
- Inequalities of health versus inequalities of health care
- Equity versus efficiency
- Needs versus wants
- Prices versus rationing
- Financial protection versus quality of life
- Public versus private
- Agents versus principals
- Universality versus selectivity
- Comprehensiveness versus limited benefit bundles
- Centralisation versus decentralisation
- Competition versus collaboration
- Experts versus citizens
- Mixing values and other things
- Key messages
Cost is also a value and no mere matter of accountancy. If we introduce a newMany politicians don't want to hear such messages. I stronlgy suggest you to read this booklet from Kings' Fund.
health care procedure, the cost will have to come out of expenditure elsewhere
in the NHS –unless there is a concurrent increase in the NHS budget. But less
expenditure elsewhere will normally imply reduction of service elsewhere and
a consequential health loss. The true cost of getting more care (and hence
health) in one area of activity is therefore the minimum necessary loss of care
(and loss of health) elsewhere. This is the important notion of opportunity cost.
.
03 d’abril 2014
Cost-effectiveness as a proxy of value
GUIA I RECOMANACIONS PER A LA REALITZACIÓ I PRESENTACIÓ D'AVALUACIONS ECONÒMIQUES I ANÀLISIS D'IMPACTE PRESSUPOSTARI DE MEDICAMENTS EN L’ÀMBIT DEL CATSALUT
As resources are scarce we do have to prioritise. That's it, we can't escape. We do need a proxy to assess relative incremental value of the technologies and procedures for a disease, otherwise decisions would be arbitrary. In such situation a methodologic guide is welcome to provide credible information. This is precisely what the guide by CatSalut is contributing to. It explains criteria and ways to present economic evaluation and budget impact analysis. A well designed guide that unfortunately right now will have a limited application. The reason is that government can't completely decide about it. It's an issue of months.
As resources are scarce we do have to prioritise. That's it, we can't escape. We do need a proxy to assess relative incremental value of the technologies and procedures for a disease, otherwise decisions would be arbitrary. In such situation a methodologic guide is welcome to provide credible information. This is precisely what the guide by CatSalut is contributing to. It explains criteria and ways to present economic evaluation and budget impact analysis. A well designed guide that unfortunately right now will have a limited application. The reason is that government can't completely decide about it. It's an issue of months.
02 d’abril 2014
Unsafe medical devices regulation
Improving Medical Device Regulation: The United States and Europe in Perspective
The regulatory differences between Europe and US are quite well known since the breast implants scandal. A US citizen was not able to receive such implant because FDA had not approved. The rationale is not related to such a case, it is the current system of notified bodies that really doesn't protect population health. However, US needs also to improve. Milbank Quarterly article says:
PS. Milbank says it is an original investigation, you may check the same title and authors some months before in Value in Health
The regulatory differences between Europe and US are quite well known since the breast implants scandal. A US citizen was not able to receive such implant because FDA had not approved. The rationale is not related to such a case, it is the current system of notified bodies that really doesn't protect population health. However, US needs also to improve. Milbank Quarterly article says:
Overall, US and European evidence requirements for devices introduce not only risks to patients but also the wrong incentives to generate the needed evidence to better understand and evaluate the benefits and risks of new devices. Considering that manufacturers often take advantage of existing evidence from already marketed devices to gain approval for a new device, they are reluctant to undertake new clinical studies. In addition, because later devices may be able to claim equivalence, the first manufacturer to market does not have a very strong incentive to undertake extensive clinical studies.The steps to improve regulation are detailed in the article. Surprisingly, notified bodies is again the chosen option in the current review of the legislation. Citizens should know it before voting.
PS. Milbank says it is an original investigation, you may check the same title and authors some months before in Value in Health
01 d’abril 2014
The foundations of a Health Policy consensus
Last Friday in Parliament, a document reflecting the foundations of a health policy consensus was presented. As a coordinator I gave a short speech highlighting salient features of the agreement. This is what I said:
I'm really convinced about the relevance of such consensus. From now on, Parliament will have to achieve a final agreement among the parties. Let's wait for a successful closing.
PS. Afterwards I was interviewed at 8TV.

Molt Honorable Presidenta del Parlament de Catalunya, Honorable Conseller, Il.lustríssims diputats, autoritats i membres de la comissió.El fet que ens reuneix avui aquí és donar resposta a la Moció 3/X adoptada en aquest Parlament per la qual s’instava al Govern a lliurar un document de bases que definís com havia de configurar-se el Sistema Nacional de Salut . El Govern de la Generalitat va aprovar el 21 de maig passat la creació de la Comissió amb aquest objectiu formada per representats del grups parlamentaris i els membres del Consell Català de la Salut.
És per això doncs que venim a presentar-vos els resultats dels treballs que hem realitzat en aquests mesos i són la mostra d’un consens entorn de vuit àmbits clau del sistema públic de salut: el finançament i la cobertura, els professionals, les prestacions i el catàleg de serveis, el model de serveis, l’avaluació, rendiment de comptes i transparència, compromís ciutadà, recerca i innovació i governança.En cadascun d’ells hem mantingut un debat ampli i obert. Hem volgut concretar principis i criteris que cal respectar i tenir en compte. Hem evitat entrar en els instruments concrets que cal utilitzar per a dur-los a terme, en la mesura que vam considerar que corresponia als responsables polítics i gestors de cada moment. Hem tractat de fixar-nos en aquells aspectes que més preocupen a la ciutadania.
La salut es troba al capdamunt de les prioritats de tota persona i sabem que al costat de compromís individual convé que els poder públics siguin capaços de d’oferir respostes col·lectives per una millor salut poblacional. És en aquest sentit que voldria seleccionar i destacar algunes de les 83 propostes que es mostren al document.
En l’àmbit de Finançament i cobertura s’assenyala amb claredat l’opció per un accés universal de la ciutadania al Sistema Nacional de Salut i alhora s’estableix un criteri de nivell de finançament públic en salut suficient i sostenible, que es relacioni amb el nivell de riquesa del país i que convergeixi amb la despesa de països amb producte interior brut per càpita equivalent i sistema sanitari similar.
En l’àmbit dels professionals s’ha considerat que la planificació de necessitats de professionals, les competències i capacitats acreditades han de ser objecte reconsideració atenent als canvis sociodemògràfics, econòmics i tecnològics. S’explicita l’èmfasi en el professionalisme com a criteri que guia la relació entre professionals amb la ciutadania, amb el sistema sanitari i els proveïdors, i la necessitat d’establir mecanismes per tal de fer efectiva la participació dels professionals en l’elaboració de polítiques i la gestió.
En l’àmbit relatiu a prestacions, s’ha considerat que cal un catàleg bàsic que respecti els criteris de seguretat, evidència científica, cost-efectivitat i avaluació d’impacte pressupostari, que és rellevant tenir en compte tant l’atenció sanitària com les intervencions comunitàries de salut pública. La garantia d’equitat d’accés a les prestacions amb qualitat cal preservar-la davant tota necessitat de salut.
En l’àmbit de model de serveis es té en compte quins han de ser els elements clau, en primer lloc les estratègies de promoció, protecció de la salut i prevenció de la malaltia, integrar las salut pública i comunitària en el model assistencial. Es mostra la rellevància de l’accessibilitat, de la gestió de casos i de la integració assistencial, així com el reforç a l’atenció primària dotant-la de més capacitat resolutiva.
En aquest àmbit també s’explicita la necessitat de respectar un conjunt de criteris en la relació contractual entre el finançador i el proveïdor, com per exemple explicitar l’orientació als resultats de salut i qualitat assistencial, la transparència interna i externa dels contractes i resultats, i els incentius a l’eficiència. Es demana d’elaborar i aplicar una normativa reguladora de la provisió d’activitat privada en els centres del SISCAT que ha de contemplar un codi ètic, una regulació de preus de prestacions complementàries, i mecanismes de controls i transparència.
En l’àmbit sobre rendiment de comptes es mostren un conjunt de mesures per tal de fer efectiva la difusió d’informació que contribueixi a la generació de coneixement i millors presa de decisions.
En l’àmbit de compromís ciutadà es destaca el paper del ciutadà com agent actiu del sistema de salut, sobre la presa de decisions compartides en tots els processos de malaltia i en especial al final de la vida.
En l’àmbit de recerca s’assenyala la importància d’optimitzar els recurs i alhora promoure noves fonts de finançament per a projectes.
En l’àmbit de governança es revisen les funcions entre diferents organismes i les seves responsabilitats, el paper del Departament cm a responsable de les polítiques sanitàries, el Servei que garanteix la cobertura i assigna els recursos i els avalua, les entitats proveïdores que ofereixen serveis sanitaris a la població. Es demana l’elaboració d’un codi de governança per a les institucions sanitàries i s’estableixen criteris per la designació d’integrants dels òrgans de govern de les institucions.
Cal dir doncs que aquestes 83 propostes mereixen una lectura detallada. El treball de col·laboració esmerçat ha estat ampli i exemplar. Avui donant resposta al mandat unànime del Parlament de Catalunya, els representants de pacients i usuaris, dels col·legis professionals, d’associacions empresarials, entitats municipalistes, societats científiques, universitats, i grups parlamentaris de CiU i ERC, us presentem aquest document de bases que considerem el fonament per tal que des d’aquest Parlament es faci efectiu un Pacte Nacional de Salut.
Si abans he assenyalat la salut com prioritat humana, el consens de les forces polítiques sobre el sistema de salut esdevé imprescindible. Precisament fa poques setmanes en un article al New England Journal of Medicine, Anne Mills revisava les característiques que tenen els sistemes sanitaris més exitosos: el consens polític n’esdevé una d’elles. I jo diria la primera de totes.
En l’elaboració d’aquest document hi ha una contribució de tots els que han participat a la comissió, també d’entitats i grups polítics que avui no han pogut donar suport a aquestes propostes. He de dir-vos que pertoca a aquesta cambra el poder fer efectiu aquest consens que desitja la ciutadania, les bases perquè això sigui possible hi són només cal teixir-les acuradament i amb generositat.
Permeteu-me que com a coordinador expressi un sentiment compartit, aquest Parlament ens ha donat l’opció de mostrar el sistema sanitari que desitgem i volem agrair-ho. Això no passa cada dia, avui és un moment singular. El país es troba en un moment singular, tots ho sabem. Algunes de les respostes al sistema sanitari que desitgem rauen precisament en una capacitat d’autogovern. És així doncs que la política i la política sanitària han d’anar de bracet. Aquest és el moment de la política en majúscules, aquell on cal deixar de banda aspectes menors i concentrar-nos en allò que ens uneix.
Vull agrair al Govern la confiança dipositada en la meva persona per tal de coordinar aquesta comissió. Vaig acceptar de bon grat i vull dir-vos que n’estic molt satisfet de com hem estat capaços de dur-ho a bon terme. Crec que ha estat exemplar, a l’alçada d’un país modern i avançat. Alhora vull agrair sincerament la col.laboració i suport tècnic que he rebut des del Departament de Salut que això ha estat clau per tal que operativament funcionés.
Als membres de la comissió, dir-vos que ha estat una experiència memorable, que personalment hem trabat nous llaços d’amistat i relació i això fa un país més fort.
És amb un esperit constructiu que sabrem afrontar els reptes de la salut de la ciutadania. Desitjo que des d’aquest Parlament s’encomani d’aquest esperit, i entenc que aquestes paraules són compartides pel conjunt de membres de la comissió, per tant esperem que d’aqui en sorgeixi un proper Pacte Nacional de Salut.
I'm really convinced about the relevance of such consensus. From now on, Parliament will have to achieve a final agreement among the parties. Let's wait for a successful closing.
PS. Afterwards I was interviewed at 8TV.
26 de març 2014
Beware of recreational WGS
Clinical Interpretation and Implications of Whole-Genome Sequencing
If some weeks ago I explained the false advertisement case on nutrigenomics, now from JAMA a new alert appears on whole genome sequencing.
If some weeks ago I explained the false advertisement case on nutrigenomics, now from JAMA a new alert appears on whole genome sequencing.
Depending on sequencing platform, a median of 10% (Illumina Inc; range, 5%-34%) to 19% (Complete Genomics Inc; range, 18%-21%) of genes associated with inherited disease and a median of 9% (Illumina Inc; range, 2%-27%) to 17% (Complete Genomics Inc; range, 17%-19%) of ACMG-reportable genes were not covered at a minimum threshold for genetic variant discoveryAs far as this is the first time that such differences are reported between two alternative sequencers over the same sample, new uncertainties arise on the value of recreational genomics.
25 de març 2014
The roots of new governance
Governance in healthcare institutions
As you know, in this blog I quote canadians in many respects. Their "Board of Directors Governance handbook" is a key document for those who want to understand the role of the board in a hospital. I suggest a quick look.
However, last week there was a closer presentation of a document of interest on governance by Consorci Sanitari i Social. The focus is closely related to the current trend towards converting hybrid organizations into public ones following an accounting criteria ESA-95. Some years ago I explained the big transformation in the ownership due to accounting rules! Incredible, but true.
I have always defended management autonomy and these moves were closely related towards less autonomy and more centralization. Right now, I'm repeating the same: we do need a system that is able to introduce the right governance and management. The issue is not only management autonomy it is also a responsible governance, an issue that in the past has been forgotten many times. The document shows the partial roadmap for such evolution. I would prefer to go beyond that and begin a deep review of current ownerhip and contracting in the public system, to improve efficiency.
As you know, in this blog I quote canadians in many respects. Their "Board of Directors Governance handbook" is a key document for those who want to understand the role of the board in a hospital. I suggest a quick look.
However, last week there was a closer presentation of a document of interest on governance by Consorci Sanitari i Social. The focus is closely related to the current trend towards converting hybrid organizations into public ones following an accounting criteria ESA-95. Some years ago I explained the big transformation in the ownership due to accounting rules! Incredible, but true.
I have always defended management autonomy and these moves were closely related towards less autonomy and more centralization. Right now, I'm repeating the same: we do need a system that is able to introduce the right governance and management. The issue is not only management autonomy it is also a responsible governance, an issue that in the past has been forgotten many times. The document shows the partial roadmap for such evolution. I would prefer to go beyond that and begin a deep review of current ownerhip and contracting in the public system, to improve efficiency.
24 de març 2014
Finding consensus in health policy
One of the key features of successful health systems is to achieve wide consensus at a societal level. Citizens have to share common values on the health system that they want. Some time ago I quoted the article by Anne Mills on this topic.
Today we can confirm that the foundations for such consensus have been built. Although unions and some parties have rejected the current text, there is a wide representation of organizations of the Catalan Council of Health. From now on, the discussion will take place in Parliament.
This is good news. You may have a look at the document here and here. There are many new insights and prescriptions to be developed.
Today we can confirm that the foundations for such consensus have been built. Although unions and some parties have rejected the current text, there is a wide representation of organizations of the Catalan Council of Health. From now on, the discussion will take place in Parliament.
This is good news. You may have a look at the document here and here. There are many new insights and prescriptions to be developed.
20 de març 2014
The seed of efficient genomic sequencing
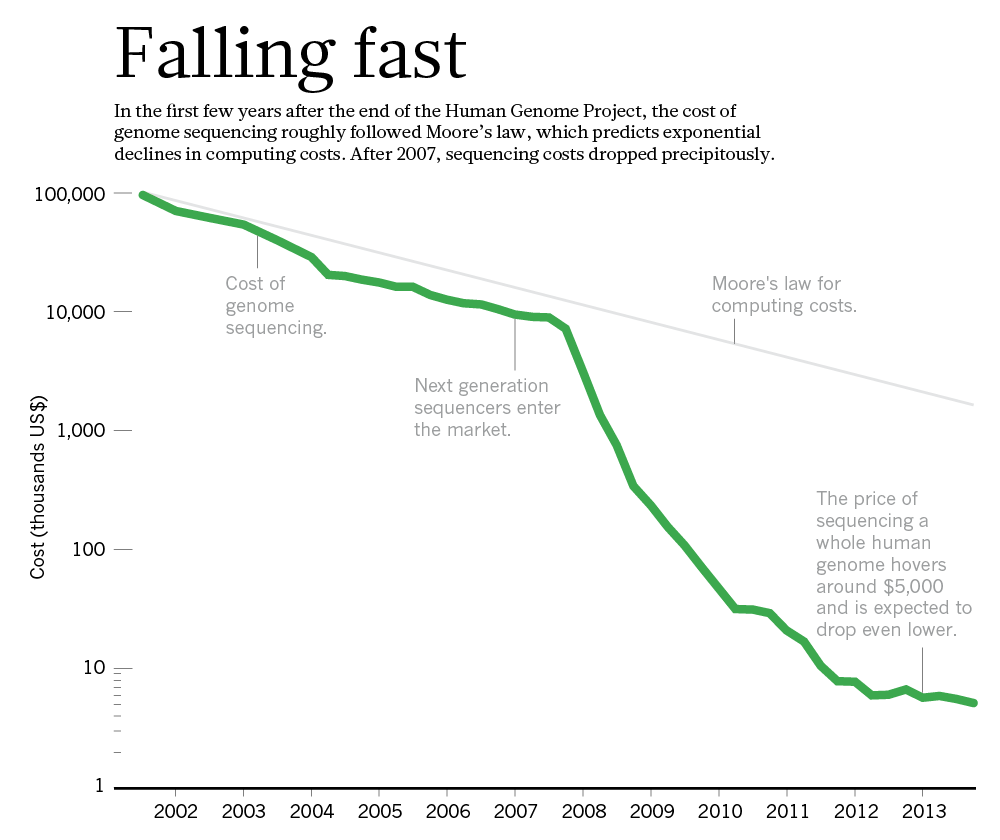
Technology: The $1,000 genome
Imagine for a moment that you have back ten years, and as the health research responsible in the government you decide to allocate $230 million to achieve a $1000 individual genome sequencing. At that moment there was a monopoly by one company, Sanger. Your effort was to promote genomic applied research, better sequencing, and doing so, the monopoly would be undermined.
This is precisely what the US government did through the Advanced sequencing technology awards and right now has achieved its aim, a more efficient sequencing. They have been extremely successful and are closing the program (NHGRI) this year: the goal has been achieved.
The funds allowed to break the former monopoly (Applied Biosystems) and at the same time, ten years later, a new quasi-monopoly has appeared (Illumina). This extraordinary story is well explained in Nature:

Imagine for a moment that you have back ten years, and as the health research responsible in the government you decide to allocate $230 million to achieve a $1000 individual genome sequencing. At that moment there was a monopoly by one company, Sanger. Your effort was to promote genomic applied research, better sequencing, and doing so, the monopoly would be undermined.
This is precisely what the US government did through the Advanced sequencing technology awards and right now has achieved its aim, a more efficient sequencing. They have been extremely successful and are closing the program (NHGRI) this year: the goal has been achieved.
The funds allowed to break the former monopoly (Applied Biosystems) and at the same time, ten years later, a new quasi-monopoly has appeared (Illumina). This extraordinary story is well explained in Nature:
Researchers are optimistic that another technology will emerge to challenge Illumina. Most think, in fact, that the crucial questions for the field will shift away from technology. Now that sequencing is cheap enough to talk about scanning every patient's genome, or at least the protein-coding portion of it, it is still not clear how that information will translate into improved care (see Nature http://doi.org/rvq; 2014). These more complex issues will require another great leap in genomic science — one that could make the trouncing of Moore's law seem easy.
PS. For those that support patents, this is a good example of how prizes substitute patents to spur innovation and confirms Mckinsey article.
19 de març 2014
Medtech on the profitable road
The 2013 Medtech Value Creators Report
Finding Sustainable Value in a Changing Market
Quick numbers from US stock exchange (2009-2013) for 65 companies in Medtech sector (medical device, medical equipment, medical supply and in vitro):
Finding Sustainable Value in a Changing Market
Quick numbers from US stock exchange (2009-2013) for 65 companies in Medtech sector (medical device, medical equipment, medical supply and in vitro):
They generated a TSR (total shareholder return) of 14.8 percent per year. While in terms of value creation its performance trails that of other health-care sectors—such as health care services (at 21.5 percent per year) and biopharmaceuticals (14.9 percent per year)—it has come with less risk (that is, a smaller spread between the TSR values of the best- and the worst-performing companies), thus offering an attractive risk-reward profile for investors.That's all folks.
18 de març 2014
Futility labeling
Choosing Wisely — The Politics and Economics of Labeling Low-Value Services
As far as the evidence on effectiveness is uncertain in some cases, somebody has to put an alert on the population. Asymetric information is always moving towards some bias and favour those with better position. This is the moment for an independent body to disseminate information towards patients. In NEJM you'll find an article about Choosing wisely, an initiative already explained in this blog. An interesting objective, although the means could be controversial. Maybe professional associations are not in best position to assume such task. Kassirer (once again) reflected many years ago the relationships with industry and their conflicts of interest. My suggestion would be independent agencies, NICE style. They should inform population about what works, and they are already doing it.
As far as the evidence on effectiveness is uncertain in some cases, somebody has to put an alert on the population. Asymetric information is always moving towards some bias and favour those with better position. This is the moment for an independent body to disseminate information towards patients. In NEJM you'll find an article about Choosing wisely, an initiative already explained in this blog. An interesting objective, although the means could be controversial. Maybe professional associations are not in best position to assume such task. Kassirer (once again) reflected many years ago the relationships with industry and their conflicts of interest. My suggestion would be independent agencies, NICE style. They should inform population about what works, and they are already doing it.
16 de març 2014
Keep on improving
On the improvement of blood sample collection at clinical laboratories
Efficiency in healthcare management comes as the result of many decisions and actions. Knowledge can improve such decisions. This weekend I was reading this article on clinical labs and how to collect samples with less routes. With operations research techniques, it is possible. Afterwards there is a need to implement them. The results of the article:
Efficiency in healthcare management comes as the result of many decisions and actions. Knowledge can improve such decisions. This weekend I was reading this article on clinical labs and how to collect samples with less routes. With operations research techniques, it is possible. Afterwards there is a need to implement them. The results of the article:
The two laboratories in this study previously planned routes manually for 43 and 74 collection points, respectively. These routes were covered by an external carrier company. With the implementation of this algorithm, the number of routes could be reduced from ten to seven in one laboratory and from twelve to nine in the other, which represents significant annual savings in transportation costsThe potential for operations research in healthcare is huge. The incentives to apply it, low (unfortunately).
13 de març 2014
Commercialism in health and medicine
Buying Health: The Costs of Commercialism and an Alternative Philosophy
There are only three topics of health policy in the newspapers (unfortunately): waiting lists, copayments and privatization. As soon as one topic drops from the agenda, the informational cascade starts with the following one. The last one, privatization is still a concept in need of definition and measurement. I already covered this issue last year and I don't want to repeat it.
Today I would like to insist that beyond a new framing of the concept, maybe we have to change the scope and the term. The right term could be commercialism. We have to understand better how and when commercialism is undermining professionalism.
Jerome Kassirer wrote an excellent piece (US oriented) in Cambridge Quarterly of Healthcare Ethics some years ago that it is still a reference for today. His words:
Churchill and Churchill go beyond the usual scope. Their recent article abstract says:
There are only three topics of health policy in the newspapers (unfortunately): waiting lists, copayments and privatization. As soon as one topic drops from the agenda, the informational cascade starts with the following one. The last one, privatization is still a concept in need of definition and measurement. I already covered this issue last year and I don't want to repeat it.
Today I would like to insist that beyond a new framing of the concept, maybe we have to change the scope and the term. The right term could be commercialism. We have to understand better how and when commercialism is undermining professionalism.
Jerome Kassirer wrote an excellent piece (US oriented) in Cambridge Quarterly of Healthcare Ethics some years ago that it is still a reference for today. His words:
Professionalism is fundamentally a pact with society. In recognition of certain behaviors and attributes, society confers professional status on us. These privileges are not bestowed, but are earned, and they must be renewed repeatedly for the status to be preserved. Professional behaviors include technical competence that is valued and that adds value, a commitment to self-improvement, a commitment to selfmonitoring and self regulation, and a commitment to use the unique knowledge and competence for the best interests of our patients. This last requirement should include a commitment to resolve conflicts of interest in our patients’ favor.
Is money trumping professionalism? Certainly the pharmaceutical money tsunami is having major adverse effects. It tends to distract faculty into emphasizing profitable research and to neglect their teaching duties. It replaces openness with secrecy, it privatizes knowledge, and it replaces part of the social commons by commercializing discovery. In many instances, it downplays knowledge as a social good. It has also created a culture within which the design of studies is sometimes jiggered to create positive results, in which unfavorable results are sometimes buried, where communication of results is sometimes hindered for commercial reasons, and where bias in publications and educational materials has gone completely uncheckedMaybe there are excessive generalizations, but take it as a general statement to be confirmed by facts and data.
Churchill and Churchill go beyond the usual scope. Their recent article abstract says:
This paper argues that commercial forces have steadily encroached into our understanding of medicine and health in modern industrial societies. The impact on the delivery of personal medical services and on common ideas about food and nutrition is profound and largely deleterious to public health. A key component of commercialization is reductionism of medical services, health products and nutritional components into small, marketable units. This reductive force makes both medical services and nutritional components more costly and is corrosive to more holistic concepts of health. We compare commercial and holistic approaches to nutrition in detail and offer an alternative philosophy. Adopting this alternative will require sound public policies that rely less on marketing as a distribution system and that enfranchise individuals to be reflective on their use of medical services, their food and nutrition choices, and their larger health needsI deeply agree with such perspective.
12 de març 2014
Against patents, again
Deadly Monopolies: The Shocking Corporate Takeover Of Life Itself – And The Consequences For Your Health And Our Medical Future
I've just finished reading a book on patents in life sciences. As you know from previous posts , I'm convinced that there is an enormous welfare loss from current patent system. If you have the opportunity to read this book, you'll finally will arrive at the same conclusion. Although it was written before the Supreme Court ruling over the Myriad case, the message is still the same: patents contrain innovation and are extremely costly to the society. The case of Hepatitis C is explained in detail. Until some patents were exhausted there was no possibility to start research. Without such patents, new succesful and (costly) treatments have arisen (and afterwards have been patented again).
An interesting interview in Forbes magazine highlights the key issues of the book. Unfortunately times go by and alternatives to patents are not taking off.
I've just finished reading a book on patents in life sciences. As you know from previous posts , I'm convinced that there is an enormous welfare loss from current patent system. If you have the opportunity to read this book, you'll finally will arrive at the same conclusion. Although it was written before the Supreme Court ruling over the Myriad case, the message is still the same: patents contrain innovation and are extremely costly to the society. The case of Hepatitis C is explained in detail. Until some patents were exhausted there was no possibility to start research. Without such patents, new succesful and (costly) treatments have arisen (and afterwards have been patented again).
An interesting interview in Forbes magazine highlights the key issues of the book. Unfortunately times go by and alternatives to patents are not taking off.
Subscriure's a:
Missatges (Atom)