Today I would like to suggest you check my previous posts on Angus Deaton, the economics Nobel prize winner. And if you have more time, a close reading of his book is required: The Great Escape: Health, Wealth, and the Origins of Inequality.
Angus Deaton deserves the prize -NYT dixit-. John Cassidy writes an excellent op-ed (The New Yorker) with the title: Angus Deaton: A Skeptical Optimist Wins the Economics Nobel. Nothing to add.
14 d’octubre 2015
09 d’octubre 2015
Using behavioral insights for policy
Social and Behavioral Sciences Team 2015 Annual Report
Some weeks ago, an executive order by President Obama boosted the application of behavioral insights to policy.

President Barack Obama speaks with members of the Social and Behavioral Sciences Team in the Oval Office in January 2015.
Some weeks ago, an executive order by President Obama boosted the application of behavioral insights to policy.
To more fully realize the benefits of behavioral insights and deliver better results at a lower cost for the American people, the Federal Government should design its policies and programs to reflect our best understanding of how people engage with, participate in, use, and respond to those policies and programs. By improving the effectiveness and efficiency of Government, behavioral science insights can support a range of national priorities, including helping workers to find better jobs; enabling Americans to lead longer, healthier lives; improving access to educational opportunities and support for success in school; and accelerating the transition to a low-carbon economy.Sounds interesting. It poses a tweak on the current approaches to policy design. Cass Sunstein says in NYT:
When government programs fail, it is often because public officials are clueless about how human beings think and act. Federal, state and local governments make it far too hard for small businesses, developers, farmers, veterans and poor people to get permits, licenses, training and economic assistance.
Behavioral research shows that efforts at simplification, or slight variations in wording, can make all the difference.The UK and now the USA are introducing this new way to define policies (and health policy). Let's keep an eye on its application and performance. What are we doing in this respect? Why are we waiting to introduce something similar?
President Barack Obama speaks with members of the Social and Behavioral Sciences Team in the Oval Office in January 2015.
07 d’octubre 2015
Cost-effectiveness of public health interventions
The case for investing in public health
The evidence shows that a wide range of preventive approaches are cost-effective, including interventions that address the environmental and social determinants of health, build resilience and promote healthy behaviours, as well as vaccination and screening. The evidence in this report shows that prevention is cost-effective in both the short and longer term. In addition, investing in públic health generates cost-effective health outcomes and can contribute to wider sustainability, with economic, social and environmental benefits.Cost-effectiveness studies are usually focused towards treatments. This report shows some examples related to public health. Unfortunately, this is not so common. Up to now my reference on this tòpic was this article. Now I'm adding this report by WHO Euro. And the question remains: if these interventions are so cost-effective, why are we waiting for their implementation?
It is recognized that a comprehensive strategy needs to include a combination of population and targeted individual preventive approaches, but it should be noted that, on average, individual-level approaches were found to cost five times more than interventions at the population level (WHO, 2011a). In general, evidence also shows that investing in upstream population-based prevention is more effective at reducing Health inequalities than more downstream prevention (Orton et al., 2011). Meanwhile, the National Institute for Health and Care Excellence in the United Kingdom found thatmany public health interventions were a lot more cost-effective than clinical interventions (using cost per QALY), and many were even cost-saving (Kelly, 2012).
03 d’octubre 2015
The healthcare funding conundrum (once again) (2)
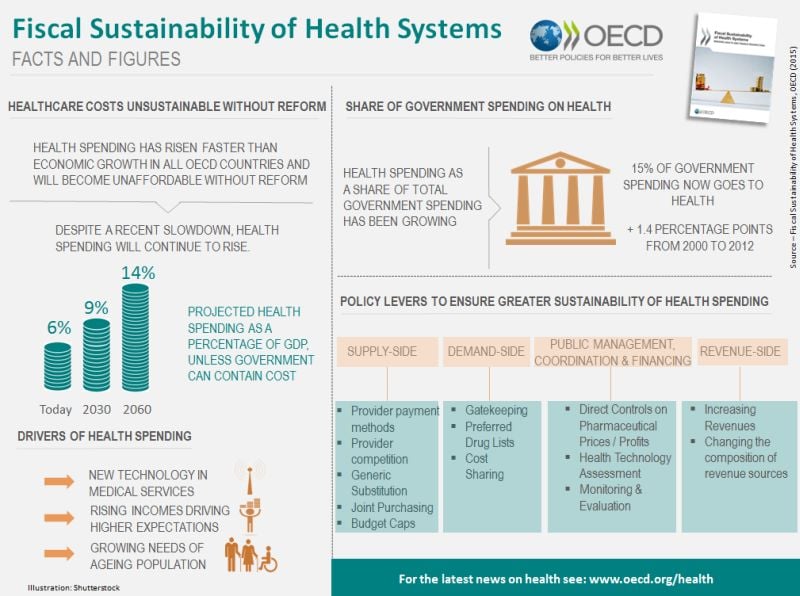
Fiscal Sustainability of Health Systems. Bridging Health and Finance Perspectives
Sustainability defined by OECD (p.25):
I understand that in some countries the budget is not credible, because its health basket is more generous and prices are higher compared to the available resources. Is this a reason to complain about cutbacks?. If there is a budget, the role of any politician is to comply with the budgetary constraint, they must prioritise. Health care is not an excuse to surpass the budget and responsible citizens and parties should acknowledge it.
Sustainability defined by OECD (p.25):
The OECD defines fiscal sustainability as the ability of a government to maintain public finances at a credible and serviceable position over the long term (OECD, 2013). Fiscal sustainability implies governments are able to maintain policies and expenditure into the future, without major adjustments and excessive debt burdens for future generations. The term refers to overall government spending, revenues, assets and liabilities that reflect past commitments and adapt to future trends such as socio-economic trends and environmental factors.
For the health sector, fiscal sustainability is perhaps best understood as a constraint that needs to be respected, rather than an objective in itself (Thomson et al., 2009). This implies that how governments achieve fiscal sustainability matters, rather than it becoming a simple cost-cutting exercise.Of course!. Sometimes OECD writes obvious statements. There is a budget constraint! Perhaps someone has forgotten it.
I understand that in some countries the budget is not credible, because its health basket is more generous and prices are higher compared to the available resources. Is this a reason to complain about cutbacks?. If there is a budget, the role of any politician is to comply with the budgetary constraint, they must prioritise. Health care is not an excuse to surpass the budget and responsible citizens and parties should acknowledge it.
02 d’octubre 2015
The healthcare funding conundrum (once again)
Fiscal Sustainability of Health Systems. Bridging Health and Finance Perspectives
Forget economic forecasts, most of them have failed many times. You don't need to be precise about the size of the GDP devoted to health in 2030, it will definitely be more expenses than now. The OECD tries in a new report to review these forecasts and to spread fear in the near future. I think that our societies before the great recession, were able to manage to some extent fiscal deficits. Now it is different, the size of the deficit for future generations is unacceptable.
The report reviews former approaches to supply side and demand side measures for cost-containment. A well known story on the macro-prescription for governments. My view is not reflected in the document. I have highlighted many times the importance of organizational change, the micro-perspective, i.e. the changes in the structure of incentives and coordination mechanisms in the health system.
This is the most challenging effort for any government, because organizational change and prioritisation represents an attempt to modify the current status quo. Governments are affraid of it, but in my opinion somebody has to handle this conundrum and tell the population exactly that unless we change current health care organizations, taxes will not be sufficient to pay the bill. Then two options will be open to us: out of pocket or no access. This is the message that this report is unable to explain clearly and now it's time for somebody to disseminate it.
PS. Read the Fiscal Sustainability of Health Systems: Policy Brief

Forget economic forecasts, most of them have failed many times. You don't need to be precise about the size of the GDP devoted to health in 2030, it will definitely be more expenses than now. The OECD tries in a new report to review these forecasts and to spread fear in the near future. I think that our societies before the great recession, were able to manage to some extent fiscal deficits. Now it is different, the size of the deficit for future generations is unacceptable.
The report reviews former approaches to supply side and demand side measures for cost-containment. A well known story on the macro-prescription for governments. My view is not reflected in the document. I have highlighted many times the importance of organizational change, the micro-perspective, i.e. the changes in the structure of incentives and coordination mechanisms in the health system.
This is the most challenging effort for any government, because organizational change and prioritisation represents an attempt to modify the current status quo. Governments are affraid of it, but in my opinion somebody has to handle this conundrum and tell the population exactly that unless we change current health care organizations, taxes will not be sufficient to pay the bill. Then two options will be open to us: out of pocket or no access. This is the message that this report is unable to explain clearly and now it's time for somebody to disseminate it.
PS. Read the Fiscal Sustainability of Health Systems: Policy Brief
26 de setembre 2015
Measuring population health
Morbilidad, utilización de recursos y costes sanitarios en la comarca del Baix Empordà
In this blog I've explained many times that if I had to pick one health system as a benchmark I would say that it is Serveis Sanitaris Integrats del Baix Empordà (SSIBE). This is my choice. I've been contributing over the last decade to understand what has happened to the morbidity, utilization and costs of this population.
Now, you have all this research effort in a PhD Dissertation by J. M. Inoriza, a must read. I strongly recommend you to have a look at it. Congratulations to all contributors.
In this blog I've explained many times that if I had to pick one health system as a benchmark I would say that it is Serveis Sanitaris Integrats del Baix Empordà (SSIBE). This is my choice. I've been contributing over the last decade to understand what has happened to the morbidity, utilization and costs of this population.
Now, you have all this research effort in a PhD Dissertation by J. M. Inoriza, a must read. I strongly recommend you to have a look at it. Congratulations to all contributors.
25 de setembre 2015
Health policy: what works?
Successes and Failures of Health Policy in Europe. Four decades of divergent trends and converging challenges
Three questions to answer:
The book was released in 2013 with data from 5 years before, an update would be necessary. Anyway, a close reading is required.
Three questions to answer:
- Do differences in rates of disease reflect differences in related policies?
- What would a country gain if it implemented the policies of the best performing country?
- Which social, economic and political factors influence a country's success in health policy?
Gains in health since 1970 for the causes analysed in this chapter have clearly been enormous. While not all of these declines can be attributed to health policies, part of the decline in all these causes can be, as shown in the previous chapters. For example, some of the declines in lung cancer and ischaemic heart disease can be attributed to tobacco control; some of the declines in external cause mortality among children to injury prevention, and some of the declines in death rate from RTIs to road safety measures, and so on. It is impossible to estimate the specific contribution of preventive health policies to these declines, but even if these accounted for only half or a quarter of the cause-specifi c declines, the successes would be immense. At the same time, not all countries have been equally successful in bringing down mortality from these preventable causes, as shown again by the calculations.
The book was released in 2013 with data from 5 years before, an update would be necessary. Anyway, a close reading is required.
Subscriure's a:
Missatges (Atom)