World report on Ageing and Health
Although it may surprise, there is no clear pattern to indicate that elderly people always utilise more health services. When one looks at the aggregated indicators, one may reach this conclusion, however taking into account the realities and individual characteristics, there are many remaining factors to explain the situation. This fact is evidenced by the last WHO report on aging and health. (P.90).
Even considering the increased morbidity at older ages, the burden of chronic diseases is diverse in terms of cost. Thus, few users and its distribution in the phase prior to death, it is the main cause of the high cost of chronic disease. Proximity to death and corresponding therapeutic effort confound the ageing factor in increasing health costs.
Furthermore, it has been shown that the compression of morbidity continues to advance. That is, the occurrence of chronic diseases is delayed gradually, the phenomenon of "survival of the fittest" is confirmed. The impact or impairment of chronic disease in human physiology for the very old is attenuated .
It is for these reasons that the report is worth, a new look to a reality that is already upon us and we need to give appropriate response.
15 d’octubre 2015
14 d’octubre 2015
A cause and consequence of progress (again)
Today I would like to suggest you check my previous posts on Angus Deaton, the economics Nobel prize winner. And if you have more time, a close reading of his book is required: The Great Escape: Health, Wealth, and the Origins of Inequality.
Angus Deaton deserves the prize -NYT dixit-. John Cassidy writes an excellent op-ed (The New Yorker) with the title: Angus Deaton: A Skeptical Optimist Wins the Economics Nobel. Nothing to add.
Angus Deaton deserves the prize -NYT dixit-. John Cassidy writes an excellent op-ed (The New Yorker) with the title: Angus Deaton: A Skeptical Optimist Wins the Economics Nobel. Nothing to add.
09 d’octubre 2015
Using behavioral insights for policy
Social and Behavioral Sciences Team 2015 Annual Report
Some weeks ago, an executive order by President Obama boosted the application of behavioral insights to policy.

President Barack Obama speaks with members of the Social and Behavioral Sciences Team in the Oval Office in January 2015.
Some weeks ago, an executive order by President Obama boosted the application of behavioral insights to policy.
To more fully realize the benefits of behavioral insights and deliver better results at a lower cost for the American people, the Federal Government should design its policies and programs to reflect our best understanding of how people engage with, participate in, use, and respond to those policies and programs. By improving the effectiveness and efficiency of Government, behavioral science insights can support a range of national priorities, including helping workers to find better jobs; enabling Americans to lead longer, healthier lives; improving access to educational opportunities and support for success in school; and accelerating the transition to a low-carbon economy.Sounds interesting. It poses a tweak on the current approaches to policy design. Cass Sunstein says in NYT:
When government programs fail, it is often because public officials are clueless about how human beings think and act. Federal, state and local governments make it far too hard for small businesses, developers, farmers, veterans and poor people to get permits, licenses, training and economic assistance.
Behavioral research shows that efforts at simplification, or slight variations in wording, can make all the difference.The UK and now the USA are introducing this new way to define policies (and health policy). Let's keep an eye on its application and performance. What are we doing in this respect? Why are we waiting to introduce something similar?
President Barack Obama speaks with members of the Social and Behavioral Sciences Team in the Oval Office in January 2015.
07 d’octubre 2015
Cost-effectiveness of public health interventions
The case for investing in public health
The evidence shows that a wide range of preventive approaches are cost-effective, including interventions that address the environmental and social determinants of health, build resilience and promote healthy behaviours, as well as vaccination and screening. The evidence in this report shows that prevention is cost-effective in both the short and longer term. In addition, investing in públic health generates cost-effective health outcomes and can contribute to wider sustainability, with economic, social and environmental benefits.Cost-effectiveness studies are usually focused towards treatments. This report shows some examples related to public health. Unfortunately, this is not so common. Up to now my reference on this tòpic was this article. Now I'm adding this report by WHO Euro. And the question remains: if these interventions are so cost-effective, why are we waiting for their implementation?
It is recognized that a comprehensive strategy needs to include a combination of population and targeted individual preventive approaches, but it should be noted that, on average, individual-level approaches were found to cost five times more than interventions at the population level (WHO, 2011a). In general, evidence also shows that investing in upstream population-based prevention is more effective at reducing Health inequalities than more downstream prevention (Orton et al., 2011). Meanwhile, the National Institute for Health and Care Excellence in the United Kingdom found thatmany public health interventions were a lot more cost-effective than clinical interventions (using cost per QALY), and many were even cost-saving (Kelly, 2012).
03 d’octubre 2015
The healthcare funding conundrum (once again) (2)
Fiscal Sustainability of Health Systems. Bridging Health and Finance Perspectives
Sustainability defined by OECD (p.25):
I understand that in some countries the budget is not credible, because its health basket is more generous and prices are higher compared to the available resources. Is this a reason to complain about cutbacks?. If there is a budget, the role of any politician is to comply with the budgetary constraint, they must prioritise. Health care is not an excuse to surpass the budget and responsible citizens and parties should acknowledge it.
Sustainability defined by OECD (p.25):
The OECD defines fiscal sustainability as the ability of a government to maintain public finances at a credible and serviceable position over the long term (OECD, 2013). Fiscal sustainability implies governments are able to maintain policies and expenditure into the future, without major adjustments and excessive debt burdens for future generations. The term refers to overall government spending, revenues, assets and liabilities that reflect past commitments and adapt to future trends such as socio-economic trends and environmental factors.
For the health sector, fiscal sustainability is perhaps best understood as a constraint that needs to be respected, rather than an objective in itself (Thomson et al., 2009). This implies that how governments achieve fiscal sustainability matters, rather than it becoming a simple cost-cutting exercise.Of course!. Sometimes OECD writes obvious statements. There is a budget constraint! Perhaps someone has forgotten it.
I understand that in some countries the budget is not credible, because its health basket is more generous and prices are higher compared to the available resources. Is this a reason to complain about cutbacks?. If there is a budget, the role of any politician is to comply with the budgetary constraint, they must prioritise. Health care is not an excuse to surpass the budget and responsible citizens and parties should acknowledge it.
02 d’octubre 2015
The healthcare funding conundrum (once again)
Fiscal Sustainability of Health Systems. Bridging Health and Finance Perspectives
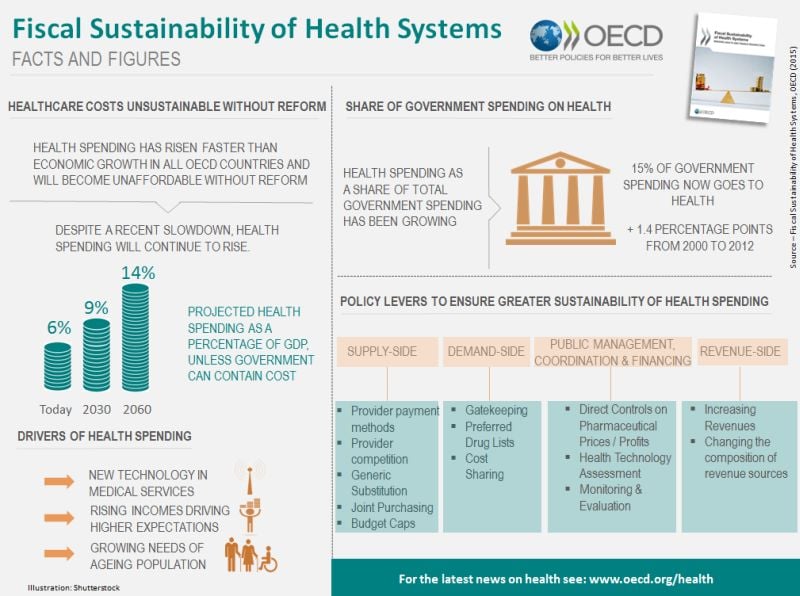
Forget economic forecasts, most of them have failed many times. You don't need to be precise about the size of the GDP devoted to health in 2030, it will definitely be more expenses than now. The OECD tries in a new report to review these forecasts and to spread fear in the near future. I think that our societies before the great recession, were able to manage to some extent fiscal deficits. Now it is different, the size of the deficit for future generations is unacceptable.
The report reviews former approaches to supply side and demand side measures for cost-containment. A well known story on the macro-prescription for governments. My view is not reflected in the document. I have highlighted many times the importance of organizational change, the micro-perspective, i.e. the changes in the structure of incentives and coordination mechanisms in the health system.
This is the most challenging effort for any government, because organizational change and prioritisation represents an attempt to modify the current status quo. Governments are affraid of it, but in my opinion somebody has to handle this conundrum and tell the population exactly that unless we change current health care organizations, taxes will not be sufficient to pay the bill. Then two options will be open to us: out of pocket or no access. This is the message that this report is unable to explain clearly and now it's time for somebody to disseminate it.
PS. Read the Fiscal Sustainability of Health Systems: Policy Brief

Forget economic forecasts, most of them have failed many times. You don't need to be precise about the size of the GDP devoted to health in 2030, it will definitely be more expenses than now. The OECD tries in a new report to review these forecasts and to spread fear in the near future. I think that our societies before the great recession, were able to manage to some extent fiscal deficits. Now it is different, the size of the deficit for future generations is unacceptable.
The report reviews former approaches to supply side and demand side measures for cost-containment. A well known story on the macro-prescription for governments. My view is not reflected in the document. I have highlighted many times the importance of organizational change, the micro-perspective, i.e. the changes in the structure of incentives and coordination mechanisms in the health system.
This is the most challenging effort for any government, because organizational change and prioritisation represents an attempt to modify the current status quo. Governments are affraid of it, but in my opinion somebody has to handle this conundrum and tell the population exactly that unless we change current health care organizations, taxes will not be sufficient to pay the bill. Then two options will be open to us: out of pocket or no access. This is the message that this report is unable to explain clearly and now it's time for somebody to disseminate it.
PS. Read the Fiscal Sustainability of Health Systems: Policy Brief
26 de setembre 2015
Measuring population health
Morbilidad, utilización de recursos y costes sanitarios en la comarca del Baix Empordà
In this blog I've explained many times that if I had to pick one health system as a benchmark I would say that it is Serveis Sanitaris Integrats del Baix Empordà (SSIBE). This is my choice. I've been contributing over the last decade to understand what has happened to the morbidity, utilization and costs of this population.
Now, you have all this research effort in a PhD Dissertation by J. M. Inoriza, a must read. I strongly recommend you to have a look at it. Congratulations to all contributors.
In this blog I've explained many times that if I had to pick one health system as a benchmark I would say that it is Serveis Sanitaris Integrats del Baix Empordà (SSIBE). This is my choice. I've been contributing over the last decade to understand what has happened to the morbidity, utilization and costs of this population.
Now, you have all this research effort in a PhD Dissertation by J. M. Inoriza, a must read. I strongly recommend you to have a look at it. Congratulations to all contributors.
25 de setembre 2015
Health policy: what works?
Successes and Failures of Health Policy in Europe. Four decades of divergent trends and converging challenges
Three questions to answer:
The book was released in 2013 with data from 5 years before, an update would be necessary. Anyway, a close reading is required.
Three questions to answer:
- Do differences in rates of disease reflect differences in related policies?
- What would a country gain if it implemented the policies of the best performing country?
- Which social, economic and political factors influence a country's success in health policy?
Gains in health since 1970 for the causes analysed in this chapter have clearly been enormous. While not all of these declines can be attributed to health policies, part of the decline in all these causes can be, as shown in the previous chapters. For example, some of the declines in lung cancer and ischaemic heart disease can be attributed to tobacco control; some of the declines in external cause mortality among children to injury prevention, and some of the declines in death rate from RTIs to road safety measures, and so on. It is impossible to estimate the specific contribution of preventive health policies to these declines, but even if these accounted for only half or a quarter of the cause-specifi c declines, the successes would be immense. At the same time, not all countries have been equally successful in bringing down mortality from these preventable causes, as shown again by the calculations.
The book was released in 2013 with data from 5 years before, an update would be necessary. Anyway, a close reading is required.
24 de setembre 2015
The modeling approach to health decisions
Applying Modeling to Improve Health and Economic Policy Decisions in the Americas: The Case of Noncommunicable Diseases
On the role of modeling in health, this OECD report says:
PS. An innovative approach with practical implications in SSIBE, Palamós.

On the role of modeling in health, this OECD report says:
In the health sector, the purpose of modeling is to structure evidence on clinical and economic outcomes in a form that can inform decisions about clinical practices and health care resource allocations. Models synthesize evidence on health consequences and costs from many different sources, including clinical trials, observational studies, insurance claim databases, case registries, public health statistics, and preference surveys. A model’s logical, mathematical framework permits the integration of facts and values and links these data to outcomes that are of interest to health care decisionmakersI agree. The report shows some examples of aggregated modeling without panel microdata. If you compare this approach with David Eddy one, Archimedes models, it is exactly the opposite. And my opinion is in favour of Archimedes, as you can check in my previous posts. The most useful approach to modeling is the one that allows improve decisions at micro level, physician and patient.
PS. An innovative approach with practical implications in SSIBE, Palamós.

Bonnard exhibition in Madrid.
19 de setembre 2015
The size of income inequality (2)

17 de setembre 2015
Epigenetics contribution to clarify disease mechanisms
Epigenetics at the Crossroads of Genes and the Environment
You may find an updated definition of epigenetics in this JAMA article:
PS. Epigenetic phenomena, from Nature.
You may find an updated definition of epigenetics in this JAMA article:
Epigenetics refers to information transmitted during cell division other than the DNA sequence per se, and it is the language that distinguishes stem cells fromIf this is so, why is the message of predictive genetics so widespread?. I've insisted on this issue before.
somatic cells, one organ from another, and even identical twins from each other. Examples include (1) DNA methylation, a covalent modification of the nucleotide cytosine, that is copied during cell division at CpG dinucleotides by the maintenance enzyme DNA methyltransferase I; (2) posttranslational modifications of nucleosome proteins about which the DNA double helix is wrapped; and (3) the density of nucleosomes and higher-order packaging of chromatin within the nucleus, including its relationship to the nuclear lamina.
The field of epigenetics and epigenetic epidemiology have much to do to improve measurement of epigenetic marks, inform natural variation in such marks, and the biological and population level relationships between genes, environment, and epigenetics. This is an important emerging area as it holds promise for better risk prediction in precision medicine as well as for clarification of disease mechanisms among the existing opaque landscape only partially informed by traditional genetic and environmental studies to date.A short and relevant article that provides hints for further reading.
PS. Epigenetic phenomena, from Nature.
16 de setembre 2015
Ownership and access to medical data
Unpatients—why patients should own their medical data
Eric Topol says in Nature Biotechnology:
PS. Hacking electronic records:
 The timeline for electronic medical data hacks in the United States of over 1 million individuals
The timeline for electronic medical data hacks in the United States of over 1 million individuals
Eric Topol says in Nature Biotechnology:
Today, in the United States, health data live in a plethora of places, from electronic health record (EHR) systems, insurance claims databases, siloed personal health apps, research and clinical trial databases, imaging files and lots of paper. Although seemingly everywhere, any true semblance of an overarching organization or standardization of medical data are lacking, whether at the individual or societal levelHis proposal is straightfoward: the ownership of the clinical record is of the patient. This situation is completely different in our country. We have public centralised repositories and the patient is the owner. There is still a lack of coordination and many things to solve, however the basics are covered in the publicly funded System, that's not the case in the private sector.
In contrast to the legal and technical difficulty an individual faces to obtain all his or her own medical data is the relative ease with which hackers have managed to breach ~100 million patient records in the first half of 2015And his proposal:
We must begin talking about creating a health data resource in a much broader and more universal context, controlled by the individuals who supply the data. This is a unique moment where we may be able to provide for personal control and, at the same time, create a global knowledge medical resource.Sounds interesting, though methodology is crucial for success.
PS. Hacking electronic records:

04 de setembre 2015
Cardiovascular disease and diabetes: progress and prospects
OECD Health Policy Studies Cardiovascular Disease and Diabetes
A recent OECD report highlights the huge improvement on cardiovascular disease and at the same time explains the policies and strategies needed for the near future. Treatment improvement accounts for 40% in the decrease of mortality, change in risk factors 50%, while 10% is unexplained. This means that public policy is critical for success. Nowadays it is still the first disease to tackle. On diabetes, the report explains that 85 million europeans are currently suffering from the disease. Therefore, it remains a severe issue.
I suggest you take a close look at the report.
A recent OECD report highlights the huge improvement on cardiovascular disease and at the same time explains the policies and strategies needed for the near future. Treatment improvement accounts for 40% in the decrease of mortality, change in risk factors 50%, while 10% is unexplained. This means that public policy is critical for success. Nowadays it is still the first disease to tackle. On diabetes, the report explains that 85 million europeans are currently suffering from the disease. Therefore, it remains a severe issue.
I suggest you take a close look at the report.
28 d’agost 2015
Healthy life expectancy: the key indicator
Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: quantifying the epidemiological transition
In former posts I have advocated that healthy life expectancy should be used as an aggregated indicator of outcomes of health determinants. Unfortunately although it is imperfect, it is the best we have, and today you can check the latest estimates in a salient article in The Lancet.
Countries with highest healthy life expectancy, both sexes, 2013
Spain has disappeared from the former top 10. I have always said that ordinal rankings have flaws, however, comparisons across time are worth taking into account.
Internally in Spain it is difficult to reverse this trend. If you consider geographic variations of the indicator you can see a range from 55 years up to 65 (p.25) .Therefore there is too much noise when you focus on the state as the unit of analysis. Forget the results and the ranking.
The only situation that is unique in the ranking is Andorra, it always appear at the top and it is a small state. That's remarkable and merits close analysis.

In former posts I have advocated that healthy life expectancy should be used as an aggregated indicator of outcomes of health determinants. Unfortunately although it is imperfect, it is the best we have, and today you can check the latest estimates in a salient article in The Lancet.
Countries with highest healthy life expectancy, both sexes, 2013
| 1 | Japan |
| 2 | Singapore |
| 3 | Andorra |
| 4 | Iceland |
| 5 | Cyprus |
| 6 | Israel |
| 7 | France |
| 8 | Italy |
| 9 | South Korea |
| 10 | Canada |
Spain has disappeared from the former top 10. I have always said that ordinal rankings have flaws, however, comparisons across time are worth taking into account.
Internally in Spain it is difficult to reverse this trend. If you consider geographic variations of the indicator you can see a range from 55 years up to 65 (p.25) .Therefore there is too much noise when you focus on the state as the unit of analysis. Forget the results and the ranking.
The only situation that is unique in the ranking is Andorra, it always appear at the top and it is a small state. That's remarkable and merits close analysis.

26 d’agost 2015
Beware of healthcare providers consolidation
The Potential Hazards of Hospital Consolidation Implications for Quality, Access, and Price
The key message:
The key message:
With the current most substantial consolidation of health care in US history, the concerning implications of the trend of hospital consolidation on quality, access, and price must be carefully considered. However, unlike banks that became too big to fail, 85% of US hospitals pay no taxes because they are designated as nonprofit organizations serving a public good. Hospitals can set prices that are ultimately passed on to others in the form of escalating insurance deductibles and taxes.The alternative:
The good work of integrated hospitals should continue to create networks of coordinated care, while at the same time, physicians and patients should insist that hospitals compete on transparent prices and quality outcomes. Achieving this goal is an important prerequisite to a functional health care system.
25 d’agost 2015
Tackling obesity: the toolbox
Patchy progress on obesity prevention: emerging examples, entrenched barriers, and new thinking
World Cancer Research Fund International NOURISHING framework
Food policy framework for healthy diets and the prevention of obesity and diet-related non-communicable diseases.

Key message:

World Cancer Research Fund International NOURISHING framework
Food policy framework for healthy diets and the prevention of obesity and diet-related non-communicable diseases.

Key message:
The problem of obesity must be reframed to acknowledge on one hand that individuals bear some personal responsibility for their health, but that, on the other hand, environmental factors exploit biological, psychological, social, and economic vulnerabilities that promote overconsumption of unhealthy foods. A vicious cycle is created in which the preference and demand for unhealthy products are not only shaped by the environment, but lead to environmental changes that further encourage consumption of unhealthy foods. This cycle makes it difficult for people to act in their own long-term self-interest, but it can be broken with regulatory actions from governments and joint efforts from industry and civil society to create healthier food systems.

07 d’agost 2015
European health regulation on lab tests, the final round?
Medical devices: Council getting ready for talks with EP
Last June 15th, there was a small but significant step towards the final agreement on Medical devices and in vitro diagnostics regulation in Europe. The need for reform has been widely requested but the lack of political consensus and the low priority given to the issue has delayed its approval in many ocasions. It seems that now is the right opportunity, however if finally passes, it will be applied on 2020!!!. It really sounds weird that it would take 5 years to be fully developed.
Anyway, if you want to have a look at the details check here and here. Right now, the lobbies are not on vacation, they are fighting against some provisions that limit their current freedom of market access. Pay attention to final result, just to check who wins and who loses, and the current state of power balance between society and the lobbies.

Last June 15th, there was a small but significant step towards the final agreement on Medical devices and in vitro diagnostics regulation in Europe. The need for reform has been widely requested but the lack of political consensus and the low priority given to the issue has delayed its approval in many ocasions. It seems that now is the right opportunity, however if finally passes, it will be applied on 2020!!!. It really sounds weird that it would take 5 years to be fully developed.
Anyway, if you want to have a look at the details check here and here. Right now, the lobbies are not on vacation, they are fighting against some provisions that limit their current freedom of market access. Pay attention to final result, just to check who wins and who loses, and the current state of power balance between society and the lobbies.

NESBITT, Lowell. Dos ponts a Nova York, 1975
06 d’agost 2015
The size of income inequality
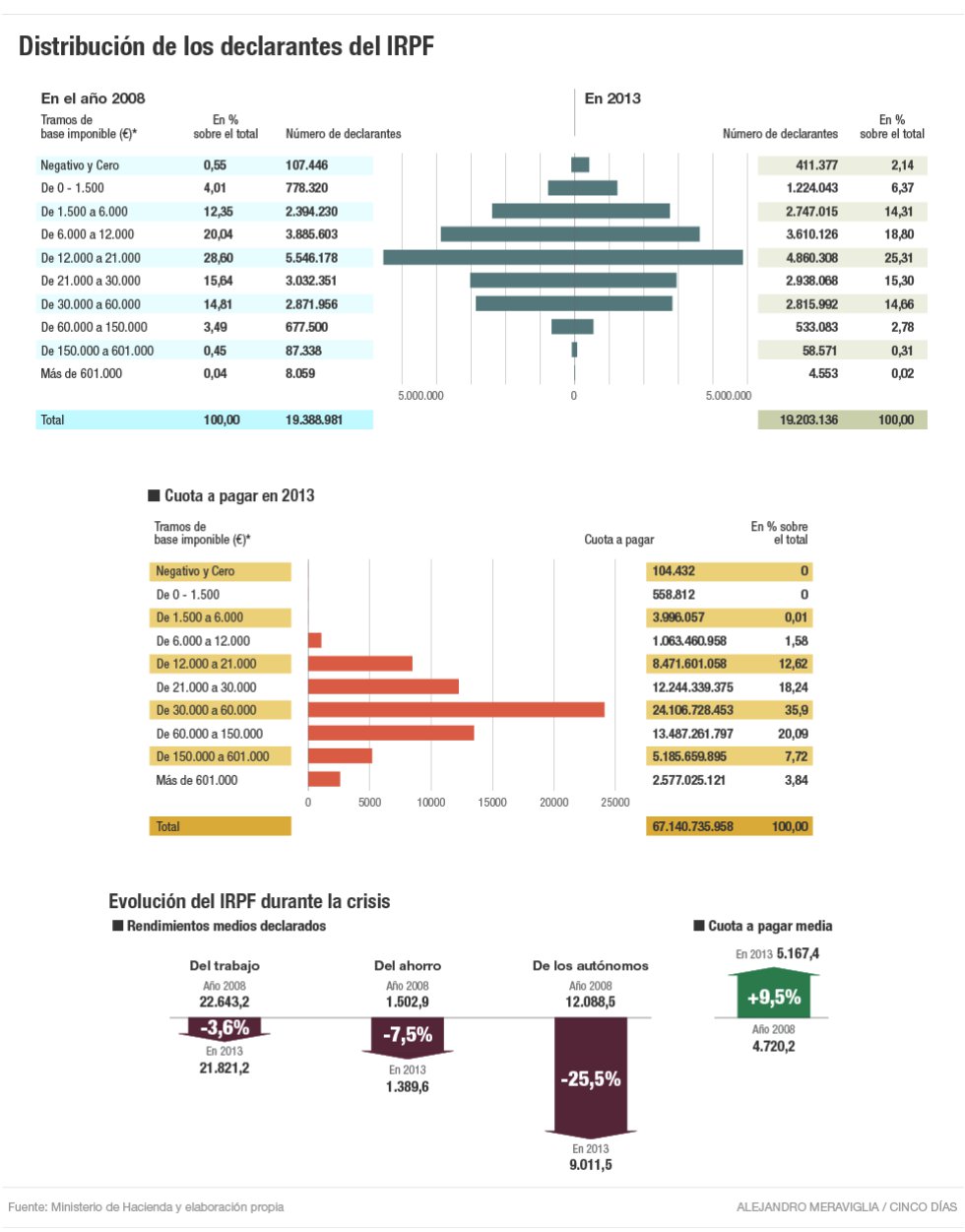
Income declared to tax authorities, not actual income. Selected statements:
- 3% of citizens account for 30% of tax collection!
- In 5 years, plutocrats have decreased by 50%!
- In 5 years, average work income has plummeted 3,6% and taxes jumped to 9,5%!
My congratulations, tax authorities!
05 d’agost 2015
04 d’agost 2015
Stratified medicine: defining the size of the market
Trusheim and Berndt provide an excellent overview of the economics of stratified medicine. I have reviewed the topic before and specifically in this post. An ideal companion diagnostic perfectly identifies and distinguishes treatment responders from those who will not.Unfortunately, in practice no diagnostic performs ideally. All diagnostics experience some level of error. In the case of a companion diagnostic, some patients will receive false positive results, scores indicating they will respond, but will not when treated. Other patients will receive false negative results, scores indicating they will not respond, but if treated they would.
So what? The key issue is about the setting of the cut-off that will define the size of the market:
Under competition, three essentially identical drugs may receive dramatically different labels, incremental cost-effectiveness ratio (ICER) justified pricing, and market positioning depending on their stratification approach. It appears superior to use an imperfect biomarker to none at all. It is less obvious whether patients, payers and firms prefer the same cut-off values for the companion diagnostic, or even whether each stakeholder a priori prefers the high, low or perhaps some other CDx cut-off value.The implications for regulating and financing of companion diagnostics are immediate. In Europe current legislation is as old as of 1998, the year that Herceptin entered into the market and the begining of stratified medicine. New regulation is still pending and there are no perspectives about a unified approach to lab tests assessment. European regulator is still on vacation.
The competing development teams may face a version of the game theory ‘prisoner’s dilemma’ in which the optimal result for patients and all firms would be to select a low or mid companion diagnostic cut-off value but the advantages of a potentially differentiating high efficacy claim may drive developers to select a high cut-off value. If all choose this approach, overall value may be reduced with many patients excluded from treatment. But the potential advantage of a higher cut-off value may prove too alluring, or the fear of a competitor selecting one, may drive all to do so. Each situation will depend on the specific facts of the indication, therapeutic, companion diagnostic and competitors
03 d’agost 2015
Lab on a chip concept, the future of diagnostics?
Future vision: next generation lab on chip concept from imec on Vimeo.
Imec develops the next generation of “lab on a chip” concepts. The idea is that such a disposable chip could be loaded with a sample of blood, saliva or urine and then quickly analyzed using a smartphone, tablet or computer, making diagnostic testing faster and easier for applications such as disease monitoring and management, disease surveillance, rural health care and clinical trials.
30 de juliol 2015
The market for health insurance price comparison
Internet has provided multiple option for price comparison through website aggregators. On health insurance you can find several alternatives. Is this market competitive? Who wins and who losses?. This is the question asked in a recent article in The Economist:
Consumers should celebrate that; the firms’ losses are their gains. But there is a catch. Comparison sites, whether for insurance or something else, introduce a new layer of costs, including their own splashy advertising campaigns. In theory, competition in the market for comparison sites ought to keep those costs down. But in a recent paper, David Ronayne of Warwick University argues that consumers often lose out from comparison sites. They earn a commission for each shopper who uses them to buy insurance. That referral cost is incorporated into the price the consumer ends up paying. If the increased costs outweigh the saving the comparison enables, consumers end up worse off.And the proposal:
How can you ensure the market for price comparison is competitive? Asking consumers to check multiple websites defeats the point of using them. One solution is to have only one site, but regulate it as a public utility. Alternatively, the government could run the site itself—much as the American government now runs comparison websites for health insurance under Obamacare.I think that this is the right approach, why not apply it here?
28 de juliol 2015
Regulating sugar sweetened beverages
Searching for Public Health Law’s Sweet Spot: The Regulation of Sugar-Sweetened Beverages
Nowadays, obesity prevention lies at the heart on any public health policy. If sugar sweetened beverages contribute decisively to obesity, then something should be done. What?. A recent PLOS article explains the options:
PS. My former posts on the same topic.
PS. Article: The impact of sugar sweetened beverages on depression risk in adults.
PS. Report: Scenarios of Macro-economic Development for Catalonia on Horizon 2030
PS. Report: FBBVA Essential Public Services.
PS. Report: Chronicle of a premeditated offensive.
Nowadays, obesity prevention lies at the heart on any public health policy. If sugar sweetened beverages contribute decisively to obesity, then something should be done. What?. A recent PLOS article explains the options:
The main regulatory approaches are taxes, restrictions on the availability of SSBs in schools, restrictions on advertising and marketing, labeling requirements, and government procurement and benefits standards.On taxes:
Savvy regulatory design has tremendous potential. For example, there is growing evidence that taxes that are more salient to consumers, such as those included in a good’s posted price (rather than being levied at the register), are more likely to influence purchasing behaviorOn public procurement, a practical suggestion for immediate application:
Restrictions on which beverages may be purchased using government funds are a less visible form of regulation, but one with potential to change the consumption patterns of large numbers of people. Outside public schools, these standards are most germane in two areas: procurement standards for public institutions (e.g., government agencies, hospitals, and prisons) and restrictions on what recipients of government benefits for the indigent may buy with those funds.
The UK’s Government Buying Standards prohibit central government bodies from procuring SSBs larger than 330 ml and encourage the wider public sector to follow the guidelines. Massachusetts and many US counties and cities have adopted nutrition standards for government contracts, but most apply to a limited set of institutions, such as childcare facilities or youth centers.
PS. My former posts on the same topic.
PS. Article: The impact of sugar sweetened beverages on depression risk in adults.
PS. Report: Scenarios of Macro-economic Development for Catalonia on Horizon 2030
PS. Report: FBBVA Essential Public Services.
PS. Report: Chronicle of a premeditated offensive.
17 de juliol 2015
Efficiency in drug patents buyout
Panning for gold: sourcing pharmaceutical innovation
Once upon a time there were pharmaceutical firms that invested mostly in internal R+D departments. Long time ago, the door was opened to contracting out, buying patents and licensing. The most recent step is to the acquisition of firms with promising molecules.
A short article in Nature sheds some light about the efficiency of recent mergers and acquisitions. And the summary is:
PS. Unfortunately, the study doesn't reflects any consideration to value in health or lobbying efforts in drug prices.
PS. FT's summer books 2015

Once upon a time there were pharmaceutical firms that invested mostly in internal R+D departments. Long time ago, the door was opened to contracting out, buying patents and licensing. The most recent step is to the acquisition of firms with promising molecules.
A short article in Nature sheds some light about the efficiency of recent mergers and acquisitions. And the summary is:
Our analysis suggests that most companies have a considerable opportunity to get better at deploying capital and resources efficiently when sourcing innovation externally. In our experience, we have found that the best performers develop robust forecasts for the key assets, are fiscally disciplined, and set up their innovation-sourcing teams and transaction capabilities to ensure that the right internal expertise is brought to bear and to ensure smooth hand‑offs through the life cycle of a deal.The success lies within, the internal expertise is crucial. Have a look at the figure and you'll notice that the most efficient (defined as the commercial impact of the products acquired relative to capital deployed in M&As) is Roche. This is not by chance.
PS. Unfortunately, the study doesn't reflects any consideration to value in health or lobbying efforts in drug prices.
PS. FT's summer books 2015
13 de juliol 2015
A closely guarded secret (2)
Direct Access Testing is the next battle for a new market for lab testing. This is at least what Theranos considers and has been lobbying for. Last December in The New Yorker there was an explanation about the firm and its goals. Afterwards JAMA added some caveats on the secretive way of conducting business and I wrote a post on that. Now The Economist has published an article with the details of the current situation about their business model.
Selling tests directly to the patient is a controversial issue. As in most of prescriptions, patients don't know enough to prescribe for themselves. However, how much is enough?. Arizona is starting to liberalise such prescriptions after Theranos successful lobbying efforts. Professional societies reflect in a position paper their perspectives on the issue.
My view is very straightforward: avoiding commercialism in health care. Under insurance coverage, prescriptions should be required after being cleared by regulators. Without insurance coverage, recreational tests have also to be licensed by regulatory authorities under a disclosure process that has not been the Theranos case. Nowadays, it still remains a secret. Selected tests could be accepted without prescription according to its implications on Health and information accuracy.
Selling tests directly to the patient is a controversial issue. As in most of prescriptions, patients don't know enough to prescribe for themselves. However, how much is enough?. Arizona is starting to liberalise such prescriptions after Theranos successful lobbying efforts. Professional societies reflect in a position paper their perspectives on the issue.
My view is very straightforward: avoiding commercialism in health care. Under insurance coverage, prescriptions should be required after being cleared by regulators. Without insurance coverage, recreational tests have also to be licensed by regulatory authorities under a disclosure process that has not been the Theranos case. Nowadays, it still remains a secret. Selected tests could be accepted without prescription according to its implications on Health and information accuracy.
08 de juliol 2015
Beware of competition in healthcare
Competition among Health Care Providers – Investigating Policy Options in the European Union
Let's imagine an official in European Commission. They are in favour of more competition in health care and asks an expert committee to assess the issue. This is the concrete answer in selected statements from the report:

Let's imagine an official in European Commission. They are in favour of more competition in health care and asks an expert committee to assess the issue. This is the concrete answer in selected statements from the report:
First, and foremost, introducing or increasing competition in the provision of health care services is a delicate policy exercise. The conditions for success and risks for failure need to be carefully assessed. In the right context, introducing competition may help to meet some health system objectives, although it is unlikely to contribute simultaneously and positively to all.Now it is crystal clear. The official has had a precise answer that it is exactly the opposite they were expecting. I've said the same in this blog several times. Take care.
Neither economic theory nor empirical evidence support the conclusion that competition should be promoted in all health services
Neither competition nor strict reliance on government regulation will solve all health system problems. Attempts to avoid or correct market failure can result in government failure and vice versa.
Provider competition can contribute to improving value in health service delivery, but details about where, when and how to introduce competition are critical. Competition in health care provision will not solve all health system problems and may have adverse effects.
Competition is unlikely to achieve improvement in all aspect of health system performance at the same time. It will not solve all the trade-offs policy makers face between different, sometimes conflicting, health system objectives.
Competition can at the same time increase the number of services provided and billed, creating uncertainty in relation to overall health care costs. That is, the introduction of competition may well result in increased costs and add to fiscal pressures. Increased costs may, or may not, be justified by additional health benefits to the population (or some parts of the population).
As competition is an instrument, sound policy evaluation studies are needed to assess and judge its effects. Such empirical studies are currently rare and even absent in some countries.
The introduction of competition has uncertain effects on equity of access to health care, as it is conditional on the effects above and on the heterogeneity of patients. Empirical work has found that the introduction of competition among hospitals, in the UK, produced little or no result in equity terms. This limited evidence does not allow for general presumptions about the effects of competition on equity of access to health care.

01 de juliol 2015
Implications of real world data
Breaking New Ground with RWE
Some decades ago evidence based medicine was the key issue in understanding effectiveness in health care and drugs. Right now the new term is Real World Evidence. You'll not find it in the wikipedia, instead I would suggest you look at this IMS report:
PS. How to introduce innovative medicines?. Have a look at this workshop.
Some decades ago evidence based medicine was the key issue in understanding effectiveness in health care and drugs. Right now the new term is Real World Evidence. You'll not find it in the wikipedia, instead I would suggest you look at this IMS report:
RWE is drawn from robust anonymous patient-level data using sound scientific and commercial analytics. It is not about amassing "Big Data" so much as performing targeted analyses on ever expanding healthcare datasets.Its impact could be large if drug prescription decisions and pricing takes into account the outcomes from the "patient journey" as they say. This is a new paradigm with uncertain spillovers. The true evidence based medicine with the power of big data. We must be aware of it and follow it closely.
While RWE is known to complement data from Randomized Clinical Trials (RCTs), its real potential is in moving decisions away from perceptions and broad extrapolations to the actual facts about patient journeys and outcomes. With innovations in data and technology, RWE is replacing other information sources such as non-behavioral primary market research (PMR), standard market reports, consumption/market data purchases, observational studies, and even selected spending on RCTs.
PS. How to introduce innovative medicines?. Have a look at this workshop.
29 de juny 2015
Organising genetic testing
Finally the government has decided to organise genetic counseling and testing. A recent instruction determines who does what. As you may remember I've said several times that government was on permanent holiday on this issue.
In this new instruction, at least two issues are forgotten: the tests that are covered, and the proliferation of sequencing instruments outside the lab. These are not minor issues.
Somebody should decide asap wether a test it is worth to be prescribed. Right now, there are no explicit constraints under the current instruction. And DNA sequencing instruments may be found in many departments under the consideration of research. If there is no clear split between research and care, I can imagine a close future with many messy labs within any hospital. Concentration of knowledge and specialisation provides wider guarantees for quality. Unless there is any mentorship program by clinical laboratories, things will go down the wrong path. Today I'm more worried than yesterday, unless these two issues are fixed.
In this new instruction, at least two issues are forgotten: the tests that are covered, and the proliferation of sequencing instruments outside the lab. These are not minor issues.
Somebody should decide asap wether a test it is worth to be prescribed. Right now, there are no explicit constraints under the current instruction. And DNA sequencing instruments may be found in many departments under the consideration of research. If there is no clear split between research and care, I can imagine a close future with many messy labs within any hospital. Concentration of knowledge and specialisation provides wider guarantees for quality. Unless there is any mentorship program by clinical laboratories, things will go down the wrong path. Today I'm more worried than yesterday, unless these two issues are fixed.
17 de juny 2015
Changing health behavior (once again)
World Development Report 2015: Mind, Society, and Behavior
Understanding human behavior is one of the main scientific endevours of our current times. As I have explained before, psychology, economics and neurosciences are making great progress in the last decades. Now the annual report by the World Bank puts all this stuff in one publication:
Understanding human behavior is one of the main scientific endevours of our current times. As I have explained before, psychology, economics and neurosciences are making great progress in the last decades. Now the annual report by the World Bank puts all this stuff in one publication:
Three principles stand out as providing the direction for new approaches to understanding behavior and designing and implementing development policy. First, people make most judgments and most choices automatically, not deliberatively: we call this “thinking automatically.” Second, how people act and think often depends on what others around them do and think: we call this “thinking socially.” Third, individuals in a given society share a common perspective on making sense of the world around them and understanding themselves: we call this “thinking with mental models".In chapter 8 you'll find the application to health issues. A clear warning:
Telling people that there is a way to improve their health is rarely sufficient to change behavior. In general, successful health promotion campaigns engage people emotionally and activate or change social norms as much as they provide information. The message disseminated should be that others will support you or even applaud you if you do it, not just that something is good for you. Successful campaigns address many or most of the following: information, performance, problem solving, social support, materials, and media . A campaign should tell people that a behavior will improve their health (information), demonstrate and model the behavior (performance), reduce barriers to its adoption (problem solving), create a system for supporting people who choose to adopt it (social support), provide the materials necessary to begin adoption (materials), and provide a background of support through in-person, print, radio, television, and other approaches (media).As you may imagine, this is much more difficult than simply giving information. This is precisely the greatest challenge.
16 de juny 2015
Health across borders
Let's think of two countries artificially separated by political borders. Both have the same income per capita (~27,700 €) and belong to the EU. The first spends 11.1 % of GDP on health (5,513€ per capita, 77.7% public funding), while the second only 8% (3,898€ per capita, 65.8% públic funding).
Both countries have roughly the same life expectancy at birth. Healthy life expectancy at 65 is better in the country that spends less. The number of visits and hospitalizations is also less. Physicians are also paid less, 18% less in general practitioners income, up to 40% in specialists income.
There is only one border between them, an artificial border created by a treaty to end a war that lasted 30 years. This is the case of part of France and Catalonia. While the first can decide over the size of resources devoted to health, the second has no role on it, by now.
PS. Today at COMB, French health reform. I'll be there. #sanitatfrança
Both countries have roughly the same life expectancy at birth. Healthy life expectancy at 65 is better in the country that spends less. The number of visits and hospitalizations is also less. Physicians are also paid less, 18% less in general practitioners income, up to 40% in specialists income.
There is only one border between them, an artificial border created by a treaty to end a war that lasted 30 years. This is the case of part of France and Catalonia. While the first can decide over the size of resources devoted to health, the second has no role on it, by now.
PS. Today at COMB, French health reform. I'll be there. #sanitatfrança
15 de juny 2015
The value of vaccination
Valuing vaccination
A PNAS article sets a broader perspective on valuing vaccines. It is of interest in light of current difteria case. My position is clear, no doubt about mandatory vaccination if its cost-effectiveness is proven.
Suggestions from the article:
Framework of vaccination benefits
A PNAS article sets a broader perspective on valuing vaccines. It is of interest in light of current difteria case. My position is clear, no doubt about mandatory vaccination if its cost-effectiveness is proven.
Suggestions from the article:
Three general recommendations flow from our arguments and related synthesis of existing evidence on broad benefits of vaccination. First, many economic evaluation studies of vaccinations should be redone to capture the full benefits generated by the vaccination in question. Second, the evidence to date on the full value of vaccination has been focused on measuring the total social benefits generated. It would also be useful to explore the distribution of vaccination’s benefits among different possible beneficiaries. Third, the primary empirical evidence on broad vaccination benefits will need to be considerably expanded and improved
Framework of vaccination benefits
| Perspective | Benefit categories | Definition | |
| Broad | Narrow | Health care cost savings | Savings of medical expenditures because vaccination prevents illness episodes |
| Care-related productivity gains | Savings of patient’s and caretaker’s productive time because vaccination avoids the need for care and convalescence | ||
| Outcome-related productivity gains | Increased productivity because vaccination improves physical or mental health | ||
| Behavior-related productivity gains | Vaccination improves health and survival, and may thereby change individual behavior, for example by lowering fertility or increasing investment in education | ||
| Community health externalities | Improved outcomes in unvaccinated community members, e.g., through herd effects or reduction in the rate at which resistance to antibiotics develops | ||
| Community economic externalities | Higher vaccination rates can affect macroeconomic performance and social and political stability | ||
| Risk reduction gains | Gains in welfare because uncertainty in future outcomes is reduced | ||
| Health gains | Utilitarian value of reductions in morbidity and mortality above and beyond their instrumental value for productivity and earnings | ||
12 de juny 2015
Reviewing the residency system
Let Me Heal. The Opportunity to Preserve Excellence in American Medicine
We usually emphasize the level of resources when we assess the results of our health system. Institutions matter, we already know that. And if there is one key success factor in our healthcare is the physician's residency program. Training of the physicians under "real" conditions has allowed substantial improvements in health outcomes and the progress of medicine that are difficult to measure specifically. In a new book, Ludmerer provides an excellent review of what it represents to US healthcare:

PS. Must see. Documentary: Big Data, citizens under scrutiny.
We usually emphasize the level of resources when we assess the results of our health system. Institutions matter, we already know that. And if there is one key success factor in our healthcare is the physician's residency program. Training of the physicians under "real" conditions has allowed substantial improvements in health outcomes and the progress of medicine that are difficult to measure specifically. In a new book, Ludmerer provides an excellent review of what it represents to US healthcare:
At the core of the residency system are fundamental educational principles: the assumption of responsibility by residents in patient management, and the importance of providing residents sufficient time to reflect and pursue subjects in depth. Also at the core are the moral principles of residency training: thoroughness, attention to detail, and learning that the needs of patients should come firstAnd considers that
The current turmoil in health care delivery offers the profession and public the opportunity to redesign medical education and practice in ways that more fully serve the needs of patients, present and future. The opportunity is there to envision medical education and practice as they should be, not as they are, and to work toward achieving that end. Such opportunities are to be treasured, not feared. The country will always need good doctors, and the medical profession has little to fear in the changes ahead as long as it remembers that it exists to serve, that the needs of patients come before its own, and that it always must be thinking of improving the future as well as caring for the present.This call for a redesign of medical education and practice is a real need in our environment. The confusion between the role of "student" and "employee" is increasing and there is no effort to clarify it.The number of physicians in the program is determined without any clear estimation of demand and rules. A total mess. That's why I consider that we should rethink it from its foundations.

PS. Must see. Documentary: Big Data, citizens under scrutiny.
09 de juny 2015
Integrated care and population health
Population health Systems: Going beyond integrated care
In this blog I have mentioned several times the works by Kindig on population health. If integrated care makes sense, it is because it improves population health. Otherwise we should talk about diferent things.
A new report by the King's Fund sheds some light on several experiences of integrated care. It's worth reading, because you'll see that there is not only one way to achieve the final goal, and the tool -better coordination- has to be suited to the specific setting.
The "recipe":
In this blog I have mentioned several times the works by Kindig on population health. If integrated care makes sense, it is because it improves population health. Otherwise we should talk about diferent things.
A new report by the King's Fund sheds some light on several experiences of integrated care. It's worth reading, because you'll see that there is not only one way to achieve the final goal, and the tool -better coordination- has to be suited to the specific setting.
The "recipe":
At a practical level, developing a population health systems perspective requires the following elements as a minimum:
• pooling of data about the population served to identify challenges and needs
• segmentation of the population to enable interventions and support to be targeted appropriately
• pooling of budgets to enable resources to be used flexibly to meet population health needs, at least between health and social care but potentially going much further
• place-based leadership, drawing on skills from different agencies and sectors based on a common vision and strategy
• shared goals for improving health and tackling inequalities based on an analysis of needs and linked to evidence-based interventions
• effective engagement of communities and their assets through third sector organisations and civil society in its different manifestations
• paying for outcomes that require collaboration between different agencies in order to incentivise joint working on population health.
FT on cancer drugs pricing
08 de juny 2015
Being aware of what's going on in marijuana market
Waiting for the opportune moment: the tobacco industry and marijuana legalization
Is it possible to prevent another public health catastrophe similar to tobacco use?. This is the question posed by a recent article in Milbank Quarterly related to marijuana legalization. They explain with complete details how:
Is it possible to prevent another public health catastrophe similar to tobacco use?. This is the question posed by a recent article in Milbank Quarterly related to marijuana legalization. They explain with complete details how:
Since at least the 1970s, tobacco companies have been interested in marijuana and marijuana legalization as both a potential and a rival product. As public opinion shifted and governments began relaxing laws pertaining to marijuana criminalization, the tobacco companies modified their corporate planning strategies to prepare for future consumer demand.And their conclusion is clear:
Policymakers and public health advocates must be aware that the tobacco industry or comparable multinational organizations (eg, food and beverage industries) are prepared to enter the marijuana market with the intention of increasing its already widespread use. In order to prevent domination of the market by companies seeking to maximize market size and profits, policymakers should learn from their successes and failures in regulating tobacco.If this is so, why does nobody care about it?. Why aren't health politicians taking decisions in the right direction?. I strongly suggest them reading this article based on the documents of the tobacco industry and act accordingly.
05 de juny 2015
What's still wrong in economics (and health economics) research
Some weeks ago I was posting on "Evidence-based economics going mainstream" , in fact the title was only taken from the book by Thaler and it is strictly a desideratum. Unfortunately what we are used every week in the university seminars is more related to Chicago style economics: Optimization +Equilibrium = Economics.
The struggle to bring academic discipline back down to earth is an unfinished business. Let's take for example this paper: Can Health Insurance Competition Work? Evidence from Medicare Advantage. The author achieves this conclusion:
Improving health is the goal, and nobody can answer to this question with this methodologic approaches. Understanding the bounded rationality, heuristics and biases of individuals is fundamental to assess any policy. As Thaler says in his book:
PS. It's not a surprise that they have forgotten a key paper on the topic by R. Frank.
PS. Must see:

The exhibition Barcelona Haggadot reunites for the first time in more than six centuries an extensive selection of these splendid works of the Catalan Gothic period that were dispersed around the world when the Jews were expelled.
Barcelona, the seat of a monarchy and a hub of Mediterranean trade, had an urban ethos that was receptive to the most innovative artistic influences in the opening decades of the 14th century. At this juncture in the Gothic era, the city’s workshops constituted a highly active centre for the production of Haggadot, manuscripts that contain the ritual of the Passover meal, which were commissioned by families living in the Call (Jewish quarter) in Barcelona and in other Jewish communities. Jews and Christians alike worked on Haggadot and shared the same style and iconographic models.
PS. Victor Grifols has recently deceased. This obituary explains clearly his commitment with health, ethics and business. RIP
The struggle to bring academic discipline back down to earth is an unfinished business. Let's take for example this paper: Can Health Insurance Competition Work? Evidence from Medicare Advantage. The author achieves this conclusion:
We estimate that private plans have costs around 12% below fee-for-service costs, and generate around $50 in surplus on average per enrollee-month, after accounting for the disutility due to enrollees having more limited choice of providers. Taxpayers provide a large additional subsidy, and insurers capture most of the private gains.Is this a conclusion?. What are the gains? Monetary gains? Does it make any sense to compare an outdated system like fee-for service with another outdated one such as "managed competition"?
Improving health is the goal, and nobody can answer to this question with this methodologic approaches. Understanding the bounded rationality, heuristics and biases of individuals is fundamental to assess any policy. As Thaler says in his book:
Moreover, much of what economists do is to collect and analyze data about how markets work, work that is largely done with great care and statistical expertise, and importantly, most of this research does not depend on the assumption that people optimize. Two research tools that have emerged over the past twenty-five years have greatly expanded economists’ repertoire for learning about the world. The first is the use of randomized control trial experiments, long used in other scientific fields such as medicine. The typical study investigates what happens when some people receive some “treatment” of interest. The second approach is to use either naturally occurring experiments (such as when some people are enrolled in a program and others are not) or clever econometrics techniques that manage to detect the impact of treatments even though no one deliberately designed the situation for that purpose. These new tools have spawned studies on a wide variety of important questions for society.There is a long way forward in economic (and health economics) research.
PS. It's not a surprise that they have forgotten a key paper on the topic by R. Frank.
PS. Must see:

The exhibition Barcelona Haggadot reunites for the first time in more than six centuries an extensive selection of these splendid works of the Catalan Gothic period that were dispersed around the world when the Jews were expelled.
Barcelona, the seat of a monarchy and a hub of Mediterranean trade, had an urban ethos that was receptive to the most innovative artistic influences in the opening decades of the 14th century. At this juncture in the Gothic era, the city’s workshops constituted a highly active centre for the production of Haggadot, manuscripts that contain the ritual of the Passover meal, which were commissioned by families living in the Call (Jewish quarter) in Barcelona and in other Jewish communities. Jews and Christians alike worked on Haggadot and shared the same style and iconographic models.
PS. Victor Grifols has recently deceased. This obituary explains clearly his commitment with health, ethics and business. RIP
04 de juny 2015
Alcohol use and abuse
Tackling Harmful Alcohol Use
Tha last OECD report is focused on health impact of alcohol and what should we do to avoid harmful effects. Key findings are the following ones:
Tha last OECD report is focused on health impact of alcohol and what should we do to avoid harmful effects. Key findings are the following ones:
- Alcohol use has both beneficial and detrimental effects on the health of individualdrinkers. At the population level, the latter outweigh the former in all countries.
- The risk of death for young male adults and young and middle-aged women increasessteadily with alcohol consumption, with no beneficial effects overall, but with relatively
- Approximately four in five drinkers would reduce their risk of death from any causes ifthey cut their alcohol intake by one unit (10 grams) per week.
- Measures of the health benefits and harms associated with alcohol use may need to
- Life years potentially gained, quality of life and individual preferences over the timing ofoutcomes are important elements in the analysis of policy options.
- Alcohol policies have to balance welfare benefits and losses. Harms to people other than drinkers are more effectively reduced by tackling heavy drinking. Price and regulation policies are more likely to affect consumer welfare.
- Harms to others, addiction, and consumers’ inaccurate perception of risk provide strong justification for government action in addressing the problem of harmful alcohol use.
03 de juny 2015
An open mind on mental health
Fit mind, fit job. From Evidence to Practice in Mental Health and Work
The social and economic impact of mental illness requires a new approach. Conventional approaches to the disease are insufficient and a broad involvement of different stakeholders is needed. These are the premises that the OECD has drawn in its new report "Fit mind, job fit. From evidence to practice in mental health and work. " While in previous reports had tried to characterize the state of affairs, now he has been concerned to review successful strategies in different countries.
The total costs of mental illness represent around 3.5% of GDP in European countries. Of this, more than half corresponds to indirect and intangible costs. Among them are productivity losses, an aspect difficult to estimate because the phenomenon of "presenteeism" appears. In the case of mental illness, the fact of going to work despite illness is the rule (over 75%) .
The issue presents differential considerations for other diseases, especially its relationship with the job and productivity. There is evidence of less satisfaction, lower quality jobs and lower pay. All contribute to conditions of work under a mental illness represent a tension for the individual and for the company. And of course in the event of unemployment, even more.
Ssome countries have tried to deal with this situation from an interdisciplinary way. That is, strictly avoiding medicalized view of health policy and trying to involve the various actors in the field of business and social environment of the patient.
The OECD recommendations fall into four areas: youth and education, business, social services and employment and healthcare. Of these, I would like to highlight here those related to the firm, being the most neglected at present.
In the field of business, strategies for supporting employees with mental health problems are crucial to achieve a positive development that avoids the end a loss of jobs and a worsening of the disease. The initial issue to consider is the detection of the problem. Somehow, managers and immediate supervisors need to provide a suitable response to the situation and often do not have the knowledge and training needed. The British example known as "Mental Health First Aid program" is a tipping point to keep in mind despite his limited success in small and medium enterprises.
The adoption of risk prevention strategies also seeks to provide tools to improve psychosocial job conditions. To this, a change of perspective in occupational medicine could contribute decisively.In cases of injury, the management of return to work eventually becomes critical for improving the stage of the disease process. To the extent that the long absences are more complex to address, it is precisely these that require attention consistently. The option of gradual return to work and support by colleagues has proven effective in this regard. The search for a negotiated solution brings more satisfactory exit routes for the disease, the conflict. And finally there are the incentive strategies and the legal obligations of employers in this regard. How to address long-term absenteeism it is a challenge in all countries and there is no rècipe for all cases. Must be combined with adequate monitoring incentives to return to the job.The uniqueness of mental illness is that the successful approach is the one that allows redevelopment activities in the labor and social environment properly. To do this, a modern approach requires among other things that the company and its employees are aware of and responsible for a different perspective and fully involved. In this direction, government and business associations should join hands to tackle an issue that so far we thought belonged only to the health system. The relevance of mental health and its impact on the welfare of citizens and their families, requires a timely response.
The social and economic impact of mental illness requires a new approach. Conventional approaches to the disease are insufficient and a broad involvement of different stakeholders is needed. These are the premises that the OECD has drawn in its new report "Fit mind, job fit. From evidence to practice in mental health and work. " While in previous reports had tried to characterize the state of affairs, now he has been concerned to review successful strategies in different countries.
The total costs of mental illness represent around 3.5% of GDP in European countries. Of this, more than half corresponds to indirect and intangible costs. Among them are productivity losses, an aspect difficult to estimate because the phenomenon of "presenteeism" appears. In the case of mental illness, the fact of going to work despite illness is the rule (over 75%) .
The issue presents differential considerations for other diseases, especially its relationship with the job and productivity. There is evidence of less satisfaction, lower quality jobs and lower pay. All contribute to conditions of work under a mental illness represent a tension for the individual and for the company. And of course in the event of unemployment, even more.
Ssome countries have tried to deal with this situation from an interdisciplinary way. That is, strictly avoiding medicalized view of health policy and trying to involve the various actors in the field of business and social environment of the patient.
The OECD recommendations fall into four areas: youth and education, business, social services and employment and healthcare. Of these, I would like to highlight here those related to the firm, being the most neglected at present.
In the field of business, strategies for supporting employees with mental health problems are crucial to achieve a positive development that avoids the end a loss of jobs and a worsening of the disease. The initial issue to consider is the detection of the problem. Somehow, managers and immediate supervisors need to provide a suitable response to the situation and often do not have the knowledge and training needed. The British example known as "Mental Health First Aid program" is a tipping point to keep in mind despite his limited success in small and medium enterprises.
The adoption of risk prevention strategies also seeks to provide tools to improve psychosocial job conditions. To this, a change of perspective in occupational medicine could contribute decisively.In cases of injury, the management of return to work eventually becomes critical for improving the stage of the disease process. To the extent that the long absences are more complex to address, it is precisely these that require attention consistently. The option of gradual return to work and support by colleagues has proven effective in this regard. The search for a negotiated solution brings more satisfactory exit routes for the disease, the conflict. And finally there are the incentive strategies and the legal obligations of employers in this regard. How to address long-term absenteeism it is a challenge in all countries and there is no rècipe for all cases. Must be combined with adequate monitoring incentives to return to the job.The uniqueness of mental illness is that the successful approach is the one that allows redevelopment activities in the labor and social environment properly. To do this, a modern approach requires among other things that the company and its employees are aware of and responsible for a different perspective and fully involved. In this direction, government and business associations should join hands to tackle an issue that so far we thought belonged only to the health system. The relevance of mental health and its impact on the welfare of citizens and their families, requires a timely response.
28 de maig 2015
The failure to find the laws of capitalism
The Rise and Decline of General Laws of Capitalism

Acemoglu and Robinson provide the best review - to my knowledge- of Piketty's work in a recent article. Their conclusion is widely shared by many people:
I do have the impression that confirmatory bias is working hard. I could say, I really believe really that Piketty has provided the argument that people wanted to hear. This is precisely the root of his success. You may read additional rationale in The Guardian. Unfortunately, there is no clear, easy and successful measure to tackle inequality - like taxing the rich, as he proposes- . I have already explained it in a former post.



Acemoglu and Robinson provide the best review - to my knowledge- of Piketty's work in a recent article. Their conclusion is widely shared by many people:
Thomas Piketty’s (2014) ambitious work proffers a bold, sweeping theory of inequality applicable to all capitalist economies. Though we believe that the focus on inequality and the ensuing debates on policy are healthy and constructive, we have argued that Piketty goes wrong for exactly the same reasons that Karl Marx, and before him David Ricardo, went astray. These quests for general laws ignore both institutions and politics, and the flexible and multifaceted nature of technology, which make the responses to the same stimuli conditional on historical, political, institutional, and contingent aspects of the society and the epoch, vitiating the foundations of theories seeking fundamental, general laws. We have argued, in contradiction to this perspective, that any plausible theory of the nature and evolution of inequality has to include political and economic institutions at the center stage, recognize the endogenous evolution of technology in response to both institutional and other economic and demographic factors, and also attempt to model how the response of an economy to shocks and opportunities will depend on its existing political and institutional equilibrium.They offer an easy proof of the most salient Piketty failure: his inability to provide any correlation between the rate of growth of the economy and the real interest rate and its impact on inequality. Acemoglu and Robinson do that and no conclusions arise.
I do have the impression that confirmatory bias is working hard. I could say, I really believe really that Piketty has provided the argument that people wanted to hear. This is precisely the root of his success. You may read additional rationale in The Guardian. Unfortunately, there is no clear, easy and successful measure to tackle inequality - like taxing the rich, as he proposes- . I have already explained it in a former post.
27 de maig 2015
Evidence-based economics going mainstream
Misbehaving. The making of Behavioral Economics
Once upon a time there was a scientific discipline created under the assumption that people choose by optimizing and that choices were rational (unbiased).
Anyway, a must-must read book. Just in the final chapter he focuses on changing the title, and he talks about evidence-based economics, rather than behavioral economics. For a health economist, this option sounds closer, since evidence-based medicine had a similar development four decades ago.
PS. Misbehaving site.
Once upon a time there was a scientific discipline created under the assumption that people choose by optimizing and that choices were rational (unbiased).
This premise of constrained optimization, that is, choosing the best from a limited budget, is combined with the other major workhorse of economic theory, that of equilibrium. In competitive markets where prices are free to move up and down, those prices fluctuate in such a way that supply equals demand. To simplify somewhat, we can say that Optimization +Equilibrium = Economics. This is a powerful combination, nothing that other social sciences can match.All these core premises of economic theory began to be under scrutiny four decades ago, with the contributions of Kahneman and Tversky on Prospect Theory and what we call right now "Behavioral Economics". Richard Tahler in his new book "Misbehaving. The making of Behavioral Economics" describes the whole history with the privilege of being on the forefront since the very begining. That's why this book is of interest. Last year another book appeared on the same topic, with a formal view: Behavioral Economics, a history. Thaler's book is of much more interest, though you can skip some details on anecdotes from several chapters. His focus on financial issues is understandable, as long as he has done most of this work in this area. However, other issues deserve more attention.
Anyway, a must-must read book. Just in the final chapter he focuses on changing the title, and he talks about evidence-based economics, rather than behavioral economics. For a health economist, this option sounds closer, since evidence-based medicine had a similar development four decades ago.
Much has changed. Behavioral economics is no longer a fringe operation, and writing an economics paper in which people behave like Humans is no longer considered misbehaving, at least by most economists under the age of fifty. After a life as a professional renegade, I am slowly adapting to the idea that behavioral economics is going mainstream. But the process of developing an enriched version of economics, with Humans front and center, is far from complete.PS. NYT review.
PS. Misbehaving site.
PS. Criticisms
PS. On Bitcoin creator: "some even suggest Nash could be Satoshi Nakamoto himself". Glups?

PS. On Bitcoin creator: "some even suggest Nash could be Satoshi Nakamoto himself". Glups?

25 de maig 2015
Hyperbolic discounting, forgotten once again
Lemons or Cherries? Asymmetric Information in the German Private Long-term Care Insurance Market
Is there adverse or advantageous selection in german private long-term care insurance market?. This is the question that addresses this article:
Is there adverse or advantageous selection in german private long-term care insurance market?. This is the question that addresses this article:
There are two predominant theories as to the effects of asymmetric information on the purchase of insurance. One theory, known as the “lemons principle”, concentrates on adverse selection, and suggests that high-risk agents choose to purchase more insurance coverage than do low-risk agents.1 A testable prediction of adverse selection theory is that risk occurrence is positively correlated with insurance coverage.The conclusion is:
The second theory as to the effects of asymmetric information concentrates on advantageous selection. This theory is also called “cherry picking”.2 Advantageous selection stresses the role of individuals’ risk aversion and argues that more risk-averse agents are both more willing to purchase insurance and more cautious.3 In the presence of advantageous selection, insurance coverage and risk occurrence are negatively correlated.
Although individuals’ self-assessment of poor health predicts their future care needs very well, such assessments are not necessarily reflected in insurance demand.In fact, these results are irrelevant as long as the effect of hyperbolic discounting has not been taken into account. Therefore, although it has been published in a widely read journal, you can skip it without any implication.
The dominating effect of adverse selection in the German private LTC insurance market gives support to the conventional claim that asymmetric information distorts market efficiency and results in lack of insurance demand.
Subscriure's a:
Missatges (Atom)