03 d’agost 2020
02 d’agost 2020

01 d’agost 2020


18 de juny 2020
Opioid crisis
Deaths of Despair and the Future of Capitalism
Beyond covid crisis there is still another one in US: the opioid crisis. The most relevant book on the topic is the Case-Deaton one.
Ps. Medicaments i risc de pneumònia
Els analgèsics opiacis causen depressió respiratòria amb la hipoventilació pulmonar resultant;
alguns d’ells (codeïna, morfina, fentanil i metadona) també tenen efectes immunosupressors.
Incrementen el risc de pneumònia i la mortalitat respiratòria en un 40 a 75%.26,27,28
L’any 2018, uns 50 milions de persones als EUA (15% de la població adulta, 25% entre els més
grans de 65 anys) reberen una mitjana de 3,4 prescripcions d’analgèsics opiacis, i 10 milions de
persones reconeixien consum exagerat d’analgèsics de prescripció mèdica.29 A Europa en els
últims anys el consum d’opiacis suaus y forts ha augmentat, sobretot entre la gent gran.30,31
Fentanil i morfina son els opiacis forts més consumits, i més recentment oxicodona. El
tramadol, que és també inhibidor de la recaptació de serotonina, és l’opiaci suau més consumit.
En dos estudis observacionals de publicació recent, el consum de tramadol, comparat amb el
d’AINE, es va associar a una mortalitat 1,6 a 2,6 vegades més alta,32,33 sobretot en pacients
amb infecció i en pacients amb malaltia respiratòria.
Beyond covid crisis there is still another one in US: the opioid crisis. The most relevant book on the topic is the Case-Deaton one.
We are telling the story in the way that we uncovered it, starting with midlife deaths of all kinds. We then focused on the immediate causes, which turned out to be deaths of despair among whites plus a slowdown and reversal in deaths from heart disease, which, until then, had been a main engine of mortality decline. Unfortunately, deaths of despair are not only afflicting middle-aged whites. While the elderly have been largely exempt, there have also been rapid increases in deaths of despair—particularly from overdoses and suicides—among younger whites. For whites between the ages of forty-five and fifty-four, deaths of despair tripled from 1990 to 2017. In 2017, this midlife age-group
had the highest rate of mortality from deaths of despair. But whites in younger age-groups were also doing badly and their deaths rose even more rapidly, accelerating in the last few years.
Drug overdoses are the single largest category of deaths of despair. They are part of a broader epidemic that includes death from alcoholism and suicide, a reflection of the social failures that we have described in this book. Yet the behavior of the pharmaceutical companies caused more deaths than would otherwise have happened, showering gasoline on smoldering despair. Stopping the drug epidemic will not eliminate the root causes of deaths of despair, but it will save many lives and should be an immediate priority. Addiction is extremely hard to treat, even with the cooperation of the addict. There appears to be wide agreement that medication-assisted treatment can be effective, but it is not available to everyone, often because of cost.
Ps. Medicaments i risc de pneumònia
Els analgèsics opiacis causen depressió respiratòria amb la hipoventilació pulmonar resultant;
alguns d’ells (codeïna, morfina, fentanil i metadona) també tenen efectes immunosupressors.
Incrementen el risc de pneumònia i la mortalitat respiratòria en un 40 a 75%.26,27,28
L’any 2018, uns 50 milions de persones als EUA (15% de la població adulta, 25% entre els més
grans de 65 anys) reberen una mitjana de 3,4 prescripcions d’analgèsics opiacis, i 10 milions de
persones reconeixien consum exagerat d’analgèsics de prescripció mèdica.29 A Europa en els
últims anys el consum d’opiacis suaus y forts ha augmentat, sobretot entre la gent gran.30,31
Fentanil i morfina son els opiacis forts més consumits, i més recentment oxicodona. El
tramadol, que és també inhibidor de la recaptació de serotonina, és l’opiaci suau més consumit.
En dos estudis observacionals de publicació recent, el consum de tramadol, comparat amb el
d’AINE, es va associar a una mortalitat 1,6 a 2,6 vegades més alta,32,33 sobretot en pacients
amb infecció i en pacients amb malaltia respiratòria.
17 de juny 2020
LATAM Health at a glance
Panorama de la Salud:Latinoamérica y el Caribe 2020
Health at a Glance: Latin America and the Caribbean 2020
This is a joint report by OECD and World Bank. It is a key reference to understand health in LATAM and Caribbean. You'll find:

Spain Health expenditure per capita 2.446 € , Cuba Health expenditure per capita 2.484 $ !!!

Health at a Glance: Latin America and the Caribbean 2020
This is a joint report by OECD and World Bank. It is a key reference to understand health in LATAM and Caribbean. You'll find:
Key indicators on health and health systems in 33 Latin America and the Caribbean countries. This first Health at a Glance publication to cover the Latin America and the Caribbean region was prepared jointly by OECD and the World Bank. Analysis is based on the latest comparable data across almost 100 indicators including equity, health status, determinants of health, health care resources and utilisation, health expenditure and financing, and quality of care. The editorial discusses the main challenges for the region brought by the COVID-19 pandemic, such as managing the outbreak as well as mobilising adequate resources and using them efficiently to ensure an effective response to the epidemic. An initial chapter summarises the comparative performance of countries before the crisis, followed by a special chapter about addressing wasteful health spending that is either ineffective or does not lead to improvement in health outcomes so that to direct saved resources where they are urgently needed.
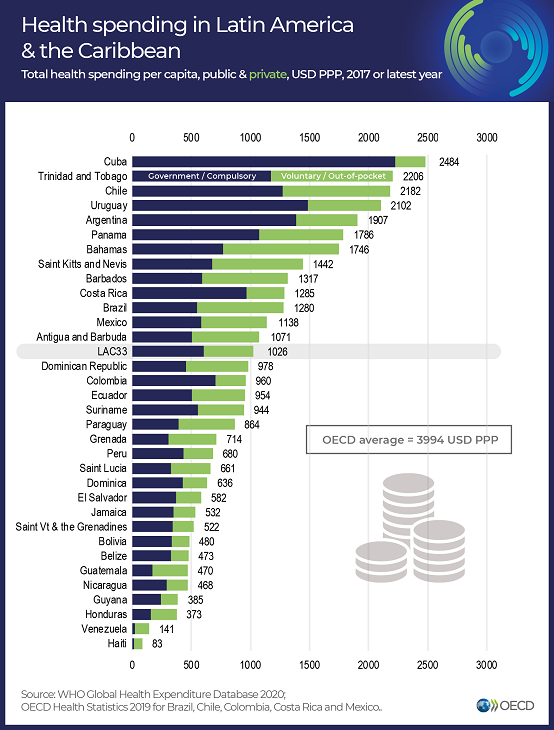
Spain Health expenditure per capita 2.446 € , Cuba Health expenditure per capita 2.484 $ !!!

16 de juny 2020
Risk adjustment, a work in progress
Risk Adjustment, Risk Sharing and Premium Regulation in Health Insurance Markets: Theory and Practice
This is a handbook on an unfinished topic. Risk adjustment is required for any managed competition model to work properly (Enthoven model) and for any funding of plans that tries to promote efficiency and avoid selection:

This is a handbook on an unfinished topic. Risk adjustment is required for any managed competition model to work properly (Enthoven model) and for any funding of plans that tries to promote efficiency and avoid selection:
The Enthoven model has evolved as its ideas have been applied in particular institutional contexts. Today, sophisticated risk adjustment models give a regulator an effective tool to quantify differences among individuals in their expected healthcare costs. Rather than a system of risk-rated premiums, regulators rely more on risk adjustment to pay plans more for higher-risk enrollees. Also, the countries in which the regulated competition model has become dominant (e.g., Germany, the Netherlands) are characterized by separation of the functions of health insurance and healthcare provision. Regulated competition can and has been implemented without the presence of integrated HMO typeTherefore, any regulator interested in mitigating health insurance market failures should read it.
risk-bearing delivery systems. In these countries, and in other settings such as Medicare Advantage in the United States, regulated competition is oriented to the health insurers, not the healthcare delivery system.
Throughout this evolution, the key feature of Enthoven’s model remains: an active collective agent on the demand side of health insurance structures and manages the health plan market to overcome market failures. Enthoven calls this agent a “sponsor,” a role that can be fulfilled by various organizations. In health insurance markets today, sponsors are mainly governments (as is common in Europe and the United States) and employers (as is common in the United States). In this volume we will generally refer to a “regulator.”
15 de juny 2020
Hospital governance: the road not taken
Effective Governance and Hospital Boards Revisited: Reflections on 25 Years of Research
There is a lot of pending work for Hospital Boards to increase its effectiveness. This article shows what has happened in the last years. However, in our close environment, things are still getting worse. Albeit, more research is needed. This is a useful framework that is applied in the article:
Table 1. Board Governance Framework for Mapping the Literature.
Research Themes
Individual actors
•• Board member
•• Board chair/officers
•• CEO/executive director
Governing bodies
•• Governing board as a body
•• Governing board subunits and affiliated
enterprises (e.g., advisory councils)
Organizations
•• Board–CEO relationship
•• Board–Organization relationship
•• Unitary and single-organization hybrids
•• Multitiered organizations
•• Organizations as actors in alliance or
network
Networks, alliances, and multiorganizational initiatives
•• Network or alliance as an organization
•• Interorganizational relationships (IOR;
when IOR is the actual focus)
•• Hybrid nonprofits–government networks
Note. Table adapted by Renz (2015) from Hambrick, Werder, and Zajac (2008) and Renz and Andersson
(2014)
There is a lot of pending work for Hospital Boards to increase its effectiveness. This article shows what has happened in the last years. However, in our close environment, things are still getting worse. Albeit, more research is needed. This is a useful framework that is applied in the article:
Table 1. Board Governance Framework for Mapping the Literature.
Research Themes
Individual actors
•• Board member
•• Board chair/officers
•• CEO/executive director
Governing bodies
•• Governing board as a body
•• Governing board subunits and affiliated
enterprises (e.g., advisory councils)
Organizations
•• Board–CEO relationship
•• Board–Organization relationship
•• Unitary and single-organization hybrids
•• Multitiered organizations
•• Organizations as actors in alliance or
network
Networks, alliances, and multiorganizational initiatives
•• Network or alliance as an organization
•• Interorganizational relationships (IOR;
when IOR is the actual focus)
•• Hybrid nonprofits–government networks
Note. Table adapted by Renz (2015) from Hambrick, Werder, and Zajac (2008) and Renz and Andersson
(2014)
14 de juny 2020
Measuring morbidity vs. measuring episodes: Two parallel views
Clinical risk groups and patient complexity: a case study with a primary care clinic in Alberta
In order to assess the health risk of a population there are two main options: Morbidity adjustment and Episodes of care. The first one can use Clinical Risk Groups, while the latter Patient focused episodes. The morbidity adjustment is useful for adjusting at population level, it is a categorical system, while episode measurement adjusts at patient level .
In this article you'll find an interesting application to a primary care center.

In order to assess the health risk of a population there are two main options: Morbidity adjustment and Episodes of care. The first one can use Clinical Risk Groups, while the latter Patient focused episodes. The morbidity adjustment is useful for adjusting at population level, it is a categorical system, while episode measurement adjusts at patient level .
In this article you'll find an interesting application to a primary care center.
CRGs have definite value with respect to predicting health care utilization, but it is important to note the limitations of the CRG as a stand-alone classification of complexity, particularly for the categorization of patients in the health status 1 throughThe article is trying to use the CRGs for episode measurement, and this is a wrong approach. CRGs are useful as a whole picture, physicians need details, only episodes can provide such information.
5 categories. In order to enhance the accuracy, relevance and predictive value of the CRG classification methodology, we see great value in pursuing methods that allow for the careful and systematic inclusion of information from the care record.
Hopper
13 de juny 2020
Why are we waiting? (5)
Waiting Times for Health Services. Next in Line

Long waiting times for health services is an important policy issue in most OECD countries. Reducing the time that people have to wait to get a consultation with a general practitioner, or a diagnostic test or treatment, can go a long way in improving patient experience and avoiding possible deterioration in their health. Governments in many countries have taken various measures to reduce waiting times, often supported by additional funding, with mixed success. This report looks at how waiting times for elective treatment, which is usually the longest wait, have stalled over the past decade in many countries, and have started to rise again in some others. It also analyses the differences in how long people have to wait to get a consultation with general practitioners or specialists across countries. The report reviews a range of policies that countries have used to tackle waiting times for different services, including elective surgery and primary care consultations, but also cancer care and mental health services, with a focus on identifying the most successful ones.Just a few words. For citizens, this is the hottest topic in our health system. And policymakers are neglecting it, while some citizens are voting with their feed...only those that can.
Bowery men waiting for bread in bread line, New York City, Bain Collection
12 de juny 2020
Primary Care value and physician compensation
Realising the Potential of Primary Health Care
If Primary Care is so important why so few physicians choose it as specialty for the residency programs?. The answer is that there is a difference in perception of value and compensation. Well, this is only the first answer. High value, high effort and low relative compensation compared to other specialties. Governments should care about it and about integrated care is finally organised. This is what OECD report says:

If Primary Care is so important why so few physicians choose it as specialty for the residency programs?. The answer is that there is a difference in perception of value and compensation. Well, this is only the first answer. High value, high effort and low relative compensation compared to other specialties. Governments should care about it and about integrated care is finally organised. This is what OECD report says:
These new models of organisation should be more widely adopted to move away from the traditional and reactive solo-practice model. While there is no one-size-fits-all model of organisation, an integrated model of primary health care often meets the following four characteristics:
Multi-disciplinary or inter-professional practices with a various mix of primary health care professionals (including GPs or family physicians, registered and advanced nurses, community pharmacists, psychologists, nutritionists, health counsellors, and non-clinical support staff), different models of teamwork, and different target populations (for example as seen in Australia, Canada, the United Kingdom and the United States) (Socha-Dietrich, 2019[101]).
Comprehensive health services in the community, (for example in Costa Rica), including disease prevention and health promotion, curative services, rehabilitation and management of chronic diseases. Care co-ordination between health professionals is key to enabling the early detection of disease, reducing the exacerbation of diseases, avoiding duplication of services, and increasing provider and patient satisfaction.
Population health management, generally based on risk stratification using sophisticated IT systems (for example in Canada and Spain), is implemented to better understand the health and risk profiles of the community and to undertake proactive management of patients’ needs. Patients are stratified to identify opportunities for intervention before the occurrence of any adverse outcomes for individual health status.
Engagement of patients in shared decision making,
Hopper
11 de juny 2020
10 de juny 2020
Precision medicine, here and now
Great article by David Cutler. The time for the returns of precision medicine has arrived in his opinion.
Precision medicine raises hopes for patients and fears for those who try to ride herd on health care spending. Will patients finally live longer and healthier lives? Will society be able to afford it? Surprisingly, at this point, personalized medicine has had less effect on both health and medical spending than either its strongest backers hoped or its most apprehensive actuaries feared.Albeit,
To date, total spending on anticancer drugs has been relatively modest. Although inflation-adjusted spending on anticancer drugs increased by $30 billion between 2011 and 2018, this is only 6% of the total increase in personal health care spending over the period. Given that administrative expenses cost an estimated 4 times the amount spent on anticancer drugs, one should be cautious about focusing excessively on the cost of precision medicine.This is a US based article, we need some estimates of our health system.
A better metric than total spending is cost effectiveness: do the benefits of the drugs outweigh the cost? The “drug abacus” tool developed by Memorial Sloan Kettering Cancer Center, which evaluates the cost-effectiveness of 52 anticancer drugs approved between 2001 and 2013, estimates that only a handful of new drugs are worth the cost at conventional valuations of life. If anticancer drugs were priced based on cost-effectiveness criteria, spending would fall by 30%.

Hopper
09 de juny 2020
Regulating voluntary health insurance
La regulació de l'assegurança voluntària de salut
Market inefficiencies can be eased with proper regulation. In a specific issue of Revista Economica de Catalunya, you'll find an article that I've written on the topic.
There is a specific and actionable proposal to improve the current situation.

Market inefficiencies can be eased with proper regulation. In a specific issue of Revista Economica de Catalunya, you'll find an article that I've written on the topic.
There is a specific and actionable proposal to improve the current situation.
Voluntary insurance in Catalonia covers 26% of citizens, possibly the most widely used duplicate insurance in Europe. Given its relevance, the regulator has to decide whether to consider the set of market failures shown in this article and act or, in contrast, put it to one side and watch its impact increase over time. For now, it is clear that government has chosen the second option.I can't summarise all details here. I suggest a close look at the article and the remaining ones in the same issue.
Considering that health is such a highly valued asset individually, surely the public deserves a satisfactory response.
Or watch this video:
Subscriure's a:
Missatges (Atom)