Forget economic forecasts, most of them have failed many times. You don't need to be precise about the size of the GDP devoted to health in 2030, it will definitely be more expenses than now. The OECD tries in a new report to review these forecasts and to spread fear in the near future. I think that our societies before the great recession, were able to manage to some extent fiscal deficits. Now it is different, the size of the deficit for future generations is unacceptable.
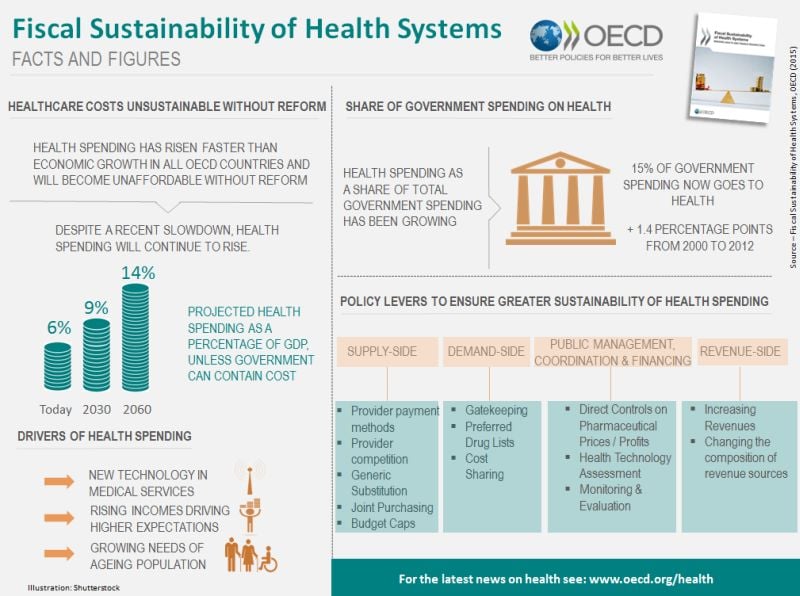
The report reviews former approaches to supply side and demand side measures for cost-containment. A well known story on the macro-prescription for governments. My view is not reflected in the document. I have highlighted many times the importance of organizational change, the micro-perspective, i.e. the changes in the structure of incentives and coordination mechanisms in the health system.
This is the most challenging effort for any government, because organizational change and prioritisation represents an attempt to modify the current status quo. Governments are affraid of it, but in my opinion somebody has to handle this conundrum and tell the population exactly that unless we change current health care organizations, taxes will not be sufficient to pay the bill. Then two options will be open to us: out of pocket or no access. This is the message that this report is unable to explain clearly and now it's time for somebody to disseminate it.
PS. Read the Fiscal Sustainability of Health Systems: Policy Brief