Sugar: Consumption at a crossroads
Should the government and health officials do more to reduce consumption of sugar, and will they in your opinion? The answer is yes, 90% of the European population consider that governments need to act, but only 52% believe the governments will do it, according to the Credit Suisse Equity Research Nutrition Survey, 2013. You'll find the details in this report.
Why so many people consider that right now something should be done about sugar intake?. Basically because everybody is increasingly convinced about the relationship between excessive sugar consumption and obesity.
The report is a good guide for all the implications and potential governmental regulation and industry self-regulation.
Definitely, something should be done, asap.
Es mostren les entrades ordenades per rellevància per a la consulta obesity. Ordena per data Mostra totes les entrades
Es mostren les entrades ordenades per rellevància per a la consulta obesity. Ordena per data Mostra totes les entrades
29 d’octubre 2013
17 de desembre 2015
A much-needed start: soda tax
Soda Politics: Taking on Big Soda (and Winning)
Obesity is a top concern on public health. Personal and collective responsibilities are linked. The concrete issue is the following one: government may require manufacturers to release information to consumers (about calories, composition, etc.), but is there anything else that he can do?
Current strategies fall short to achieve the goals of obesity reduction. Nutritional labels are not enough, are taxes an option?. Some countries have already implemented taxes on fizzy drinks, fat or salty foods. There are complex technical issues to be considered. However, The Economist says that taxes on fizzy drinks seems to work as intended. If this is really so, then there is a much-needed reason to start in this way.
Marion Nestle in her latest book "Soda Politics" provides the hole list of arguments. Any regulator should read in detail the book, specially part IX on "Advocacy: Soda caps, taxes and more", and take into account her recommendation:

PS. A must read. Understanding 25 years of health policy in Catalonia, released in this journal: Referent. You'll find an article that I have written for the occasion.
Obesity is a top concern on public health. Personal and collective responsibilities are linked. The concrete issue is the following one: government may require manufacturers to release information to consumers (about calories, composition, etc.), but is there anything else that he can do?
Current strategies fall short to achieve the goals of obesity reduction. Nutritional labels are not enough, are taxes an option?. Some countries have already implemented taxes on fizzy drinks, fat or salty foods. There are complex technical issues to be considered. However, The Economist says that taxes on fizzy drinks seems to work as intended. If this is really so, then there is a much-needed reason to start in this way.
Marion Nestle in her latest book "Soda Politics" provides the hole list of arguments. Any regulator should read in detail the book, specially part IX on "Advocacy: Soda caps, taxes and more", and take into account her recommendation:
Let me acknowledge immediately that advocacy to reduce soda intake faces special challenges that distinguish it from advocacy for reduction of alcohol, tobacco, or junk foods. Like these other industries, the soda industry sells relatively inexpensive products that are available in almost every corner of the globe. Like them, this industry is extremely wealthy. Also like the others, health is the industry’s Achilles’ heel. But in sharp contrast to companies selling junk food, alcohol, or tobacco, Coca-Cola and PepsiCo consistently rank among the most admired, respected, and honored companies in the world. Health and environmental advocates must recognize the power of this favorable public perception when encouraging others to resist it.
PS. A must read. Understanding 25 years of health policy in Catalonia, released in this journal: Referent. You'll find an article that I have written for the occasion.
21 d’abril 2017
Approaching the golden age of epigenomics and epitranscriptomics
A new twist on epigenetics
If epigenomics is crucial to discard the genetic predestination paradigm, now we can add a new 'omics to the paradigm: epitranscriptomics. Last February, Nature published interesting news related to recent scientific developments:
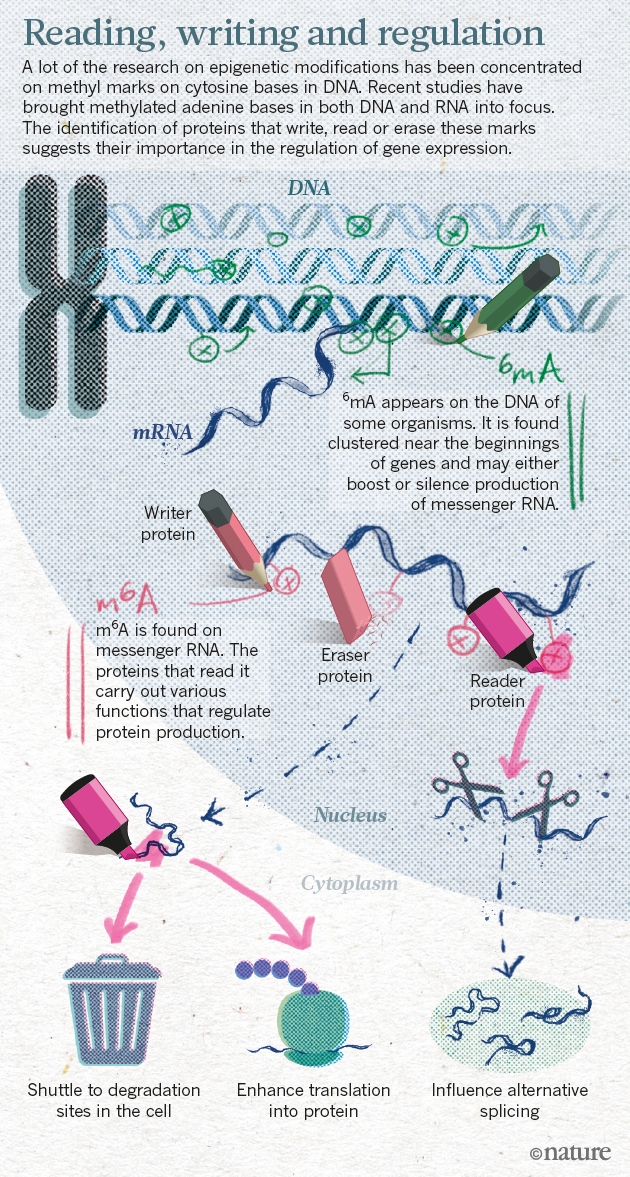
If epigenomics is crucial to discard the genetic predestination paradigm, now we can add a new 'omics to the paradigm: epitranscriptomics. Last February, Nature published interesting news related to recent scientific developments:
The epigenome helps to explain how cells with identical DNA can develop into the multitude of specialized types that make up different tissues. The marks help cells in the heart, for example, maintain their identity and not turn into neurons or fat cells. Misplaced epigenetic marks are often found in cancerous cells.Chuan He and Tao Pan are two researchers that have been working on new ways of controlling gene expression
He and others have shown that a methyl group attached to adenine, one of the four bases in RNA, has crucial roles in cell differentiation, and may contribute to cancer, obesity and more. In 2015, He’s lab and two other teams uncovered the same chemical mark on adenine bases in DNA (methyl marks had previously been found only on cytosine), suggesting that the epigenome may be even richer than previously imagined.
The team had shown for the first time that RNA methylation was reversible, just like the marks found on DNA and histones.Methylated adenine bases are the focus of research on gene expression.
20 de novembre 2013
A healthier population (after all this years)
Enquesta de salut de Catalunya 2012. Informe dels principals resultats
It is just a fact. The authors of The Lancet article were unable to have a look at the last Catalan Health Survey. In 2006, 78,6% of population considered their health as good, in 2012 (p54) this figure has moved up to 82,8%. The Lancet only emphasized negative issues without clear evidence. It seems that this is the selling argument of our times.
The most relevant thing from the health survey is that citizens view themselves healthier than before the recession, you'll find additional details inside the report.
However, a closer look may highlight some doubts about individual health behaviours, smoking by young people and specially the obesity epidemics. Therefore, a short applause and a clear public health alert for an improvement of health behaviours.
It is just a fact. The authors of The Lancet article were unable to have a look at the last Catalan Health Survey. In 2006, 78,6% of population considered their health as good, in 2012 (p54) this figure has moved up to 82,8%. The Lancet only emphasized negative issues without clear evidence. It seems that this is the selling argument of our times.
The most relevant thing from the health survey is that citizens view themselves healthier than before the recession, you'll find additional details inside the report.
However, a closer look may highlight some doubts about individual health behaviours, smoking by young people and specially the obesity epidemics. Therefore, a short applause and a clear public health alert for an improvement of health behaviours.
12 de desembre 2024
Estratègies cost-efectives per a un pes saludable
Overcoming obesity: An initial economic analysis
Els de Mckinsey van fer una anàlisi fa una dècada sobre quines eren les estratègies més cost-efectives per afrontar l'obesitat. Jo desconec en profunditat com es va arribar a aquestes dades i la dificultat metodològica és molt considerable.
Avui recupero la taula que es refereix al Regne Unit:

Desconec si encara manté la vigència. Tinc la impressió que caldria refer-ho. En una dècada han passat moltes coses, i la més recent és el paper de la semaglutida com opció. Ara estan sortint moltes avaluacions que caldrà repassar properament.
PS. Algú hauria de revisar en profunditat això i actualitzar-ho també.
03 de juliol 2014
Healthy and satisfied
Enquesta de salut de Catalunya
Latest data from the 2013 Health Survey shows that 81,1% of the population consider themselves as healthy, slightly better that in 2010 that was 79,3%. Regarding satisfaction, 86,9% of population is satisfied with public health services, again better than 2010 that was 84,7%. Though in 2012 results were a little bit better.
In the details of the results you'll find that obesity and overweight is the biggest issue to address in my opinion. There is still a lot to do on tobacco and alcohol, but data shows some improvement.
This health survey should be broadcast in the media and efforts to promote healthy behaviours should raise. Unfortunately nowadays media is focused on negative messages and this issue lies far from journalists' interests.
Latest data from the 2013 Health Survey shows that 81,1% of the population consider themselves as healthy, slightly better that in 2010 that was 79,3%. Regarding satisfaction, 86,9% of population is satisfied with public health services, again better than 2010 that was 84,7%. Though in 2012 results were a little bit better.
In the details of the results you'll find that obesity and overweight is the biggest issue to address in my opinion. There is still a lot to do on tobacco and alcohol, but data shows some improvement.
This health survey should be broadcast in the media and efforts to promote healthy behaviours should raise. Unfortunately nowadays media is focused on negative messages and this issue lies far from journalists' interests.
07 de desembre 2023
Desxifrant el rellotge vital que portem dins
Are your organs ageing well? The blood holds clues
Organ aging signatures in the plasma proteome track health and disease
L'envelliment deixa senyals a les cèl·lules i aquests canvis bioquímics provoquen danys a òrgans i poden causar finalment la mort. Saber perquè i com envellim ha esdevingut un repte per a molts investigadors, és com treballar sobre la causa de les causes de la salut. Es tracta de conèixer els canvis moleculars en els òrgans humans quan anem envellint. L'article de Lopez-Otin, Blasco i Serrano a Cell aquest gener passat mostrava una revisió àmplia de l'estat de la qüestió. Article per llegir i guardar.
Ara a Stanford han trobat la manera d'identificar proteïnes a la sang que assenyalen l'envelliment de determinats òrgans del cos. No tots els òrgans evolucionen per igual i quan un s'espatlla pot afectar un altre. Hi havia aportacions anteriors molt importants des de l'epigenoma que ja ho apuntaven. Ara bé, el que apareix ara és molt més holístic i pràctic, i l'aprenentage automàtic ha ajudat a assolir el resultat. A l'editorial de Nature diuen:
To explore how organs age, Oh and his colleagues first analysed nearly 5,000 proteins in blood samples from 1,398 healthy adults. They identified about 850 proteins that originated mainly from a single organ and trained a machine-learning algorithm to predict a person’s age on the basis of the levels of these proteins. They validated their model using blood samples from more than 4,000 other people.
The results showed that an organ’s biological age is linked to disease risk. For example, roughly 2% of participants had accelerated heart ageing — that is, their levels of blood proteins relating to heart ageing differed substantially from those of other people of the same age. Having a prematurely old heart was linked to a 250% increased risk of heart failure, the authors found.
Atès que el rellotge vital de cadascú ens diu l'edat dels òrgans, estem a punt de poder identificar amb precisió quin és el risc personal d'emmalaltir. Aquest és un salt rellevant en el coneixement, han trobat els biomarcadors dels biomarcadors.
La qüestió immediata que apareix és què cal fer amb aquesta nova informació del risc? Cal saber-la tota? Hi ha riscos mitigables? evitables?. L'entorn i els comportaments, com ajudaran a millorar i no espatllar els riscos ja existents?
PS. Grifols segueix la pista d'això, hi és al darrera. Mireu el darrer signant de l'article Wyss Coray, i la seva empresa Alkahest.
PS. Si us llegiu l'article sencer de Nature, hi trobareu detalls de molt interès, com aquest:
The kidney ageotype was the most significantly associated with metabolic diseases (diabetes, obesity, hypercholesterolaemia and hypertension), the heart ageotype was the most significantly associated with heart diseases (atrial fibrillation and heart attack), the muscle ageotype was the most significantly associated with gait impairment, the brain ageotype was the most significantly associated with cerebrovascular disease and the organismal ageotype was the most significantly associated with Alzheimer, AD.
At the population level, the two most significant associations between disease and age gap were between the kidney age gap and metabolic disease traits.
Si les proteïnes del plasma prediuen envelliment de l'òrgan i aquest prediu el risc de malaltia...aleshores ens cal conèixer com tenim les proteïnes del plasma. Ara bé, no m'interessa conèixer el risc de malalties no "accionables", no ho vull saber. Per altra banda, si que vull saber aquells riscos d'emmalaltir sobre els que puc contribuir a reduir-los o evitar-los, o aquells que l'entorn i el sistema de salut hi pot contribuir.

Robert Mapplethorpe a la Galeria Senda
17 de juny 2022

09 de desembre 2024
L'obesitat com a repte global
Obesity. Health and Economic Consequences of an Impending Global Challenge
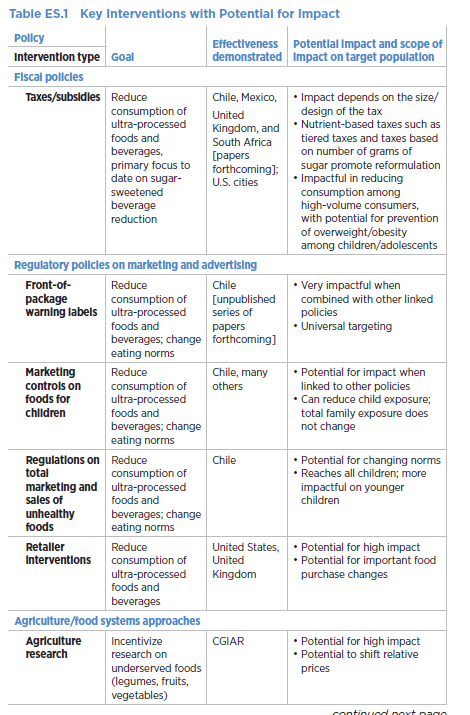
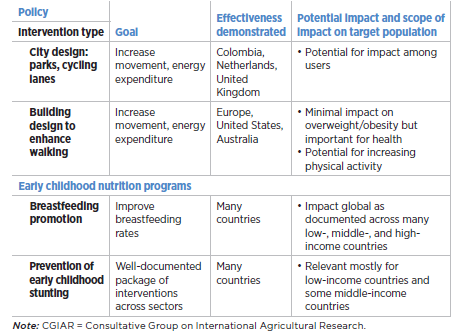
Poc abans de la pandèmia, el Banc Mundial va publicar aquest informe que em va passar per alt. Planteja l'obesitat com a repte global, i posa dades i estratègies per afrontar-lo. Cal llegir-lo, aqeusta és la infografia:

i aquesta és una taula seleccionada del que cal fer:

Ara cal que algú faci alguna cosa...
PS. Resum IA
Aquest llibre, publicat pel Banc Mundial el 2020, examina l'epidemiologia canviant del sobrepès i l'obesitat i les tendències actuals a tot el món. El llibre argumenta que el sobrepès i l'obesitat són una "bomba de rellotgeria" amb enormes impactes econòmics i sanitaris negatius potencials. Aquest problema afecta especialment els pobres i les persones que viuen en països de renda baixa o mitjana. El llibre destaca que el sobrepès i l'obesitat ja no són només un problema dels països d'alts ingressos i de les zones urbanes.
El llibre desmenteix el mite que l'obesitat és un problema només dels països d'alts ingressos i de les zones urbanes. De fet, més del 70% de les persones amb sobrepès o obesitat viuen en països de renda baixa o mitjana. A més, l'ús actual del límit d'índex de massa corporal (IMC) de 25 pot subestimar la càrrega total de sobrepès i obesitat en aquests països.
El llibre presenta una sèrie d'intervencions i polítiques prometedores per abordar el problema, com ara:
● Impostos sobre begudes ensucrades
● Etiquetatge frontal dels envasos
● Controls de màrqueting sobre aliments per a nens
● Millora del disseny urbà i revitalització
● Promoció d'una dieta saludable i activitat física
● Millora de la qualitat del sistema alimentari
● Ampliació de les intervencions prenatals i de la primera infància
El llibre també examina l'experiència de diversos països en la implementació d'aquestes polítiques, com ara Mèxic, Xile, l'Índia, Polònia, Tailàndia, Sud-àfrica, Sri Lanka i Turquia.
El llibre conclou que les institucions de desenvolupament com el Banc Mundial tenen un paper important a jugar en la promoció d'aquestes intervencions a escala mundial. No obstant això, el llibre també adverteix que aquest potencial encara no s'ha maximitzat.
El llibre demana una major investigació i anàlisi sobre:
● L'impacte de les polítiques fiscals i reguladores
● Les intervencions intersectorials
● La millor manera d'adaptar aquestes polítiques a diferents contextos de país
A més de proporcionar un resum detallat del problema de l'obesitat, el llibre ofereix una guia pràctica per als països que busquen abordar aquest repte creixent.
08 de setembre 2023
La petjada de la COVID
Trobo que no s'en parla prou de la petjada que la COVID ha deixat a alguns dels nostres cossos. L'Eric Topol se n'ha preocupat força i n'ha fet aquest resum:

I on diu Spain podeu considerar que diu Catalunya, perquè es refereix a aquest article. I la troballa després de 2 anys d'estudiar la població amb Post-Covid condition PCC, és aquesta:
The study included 548 individuals, 341 with PCC, followed for a median of 23 months (IQR 16.5–23.5), and 207 subjects fully recovered. In the model with the best fit, subjects who were male and had tertiary studies were less likely to develop PCC, whereas a history of headache, or presence of tachycardia, fatigue, neurocognitive and neurosensitive complaints and dyspnea at COVID-19 diagnosis predicted the development of PCC. The cluster analysis revealed the presence of three symptom clusters with an additive number of symptoms. Only 26 subjects (7.6%) recovered from PCC during follow-up; almost all of them (n = 24) belonged to the less symptomatic cluster A, dominated mainly by fatigue. Recovery from PCC was more likely in subjects who were male, required ICU admission, or had cardiovascular comorbidities, hyporexia and/or smell/taste alterations during acute COVID-19. Subjects presenting with muscle pain, impaired attention, dyspnea, or tachycardia, conversely, were less likely to recover from PCC.
Table 4Characteristics of the post-COVID-19 condition clusters.
| Cluster A | Cluster B | Cluster C | |
|---|---|---|---|
| N (%) | 139 (40.8) | 152 (44.6) | 50 (14.2) |
| Age, years, median (IQR) | 50 (42–57) | 47 (38–56) | 45 (39–51) |
| Sex, female, N (%) | 73 (52.5) | 120 (78.9) | 45 (90) |
| Hospitalization, N (%) | 65 (46.8) | 52 (34.2) | 13 (26) |
| Intensive care, N (%) | 10 (7.2) | 5 (3.3) | 1 (2) |
| Comorbidities, N (%) | |||
| Allergy | 31 (22.3) | 56 (36.8) | 20 (40) |
| Obesity | 32 (23.0) | 39 (25.7) | 13 (26.0) |
| Dyslipidemia | 30 (21.6) | 43 (28.3) | 9 (18.0) |
| Hypertension | 34 (24.5) | 25 (16.4) | 8 (16.0) |
| Lung disease | 21 (15.1) | 31 (20.4) | 6 (12.0) |
| Persistent symptoms, N (%) | |||
| Fatigue | 100 (71.9) | 139 (91.4) | 48 (96.0) |
| Neurocognitive complaints | 62 (44.6) | 128 (84.2) | 46 (92.0) |
| Dyspnea | 45 (32.4) | 131 (86.2) | 44 (88.0) |
| Headache | 41 (29.5) | 103 (67.8) | 44 (88) |
| Myalgia | 31 (22.3) | 98 (64.5) | 33 (66) |
| Arthralgia | 39 (28.1) | 92 (60.5) | 47 (94) |
| Chest pain | 31 (22.3) | 76 (50.0) | 45 (90) |
| Tachycardia | 19 (13.7) | 83 (54.6) | 39 (78.0) |
| Cough | 18 (12.9) | 64 (42.1) | 19 (38.0) |
| Neurosensitive symptoms | 31 (22.3) | 66 (43.4) | 40 (80.0) |
| Diarrhea | 14 (10.1) | 59 (38.8) | 26 (52.0) |
| Low grade fever | 13 (9.35) | 36 (23.7) | 21 (42.0) |
| Smell alterations | 34 (24.5) | 38 (25) | 30 (60) |
| Dermatological alterations | 24 (17.3) | 36 (23.7) | 43 (86) |
| Dysphagia | 9 (6.47) | 18 (11.8) | 27 (54) |
| Dysphonia | 10 (7.19) | 29 (19.1) | 19 (38) |
| Recovery from PCC, N (%) | 24 (17.3) | 1 (0.7) | 1 (2.0) |
I la petjada després de dos anys persisteix encara en bona part de la població amb PCC. I moltes coses que encara no sabem...
20 de novembre 2011
L'economia del comportament i l'obesitat
Eating Behavior and Obesity Behavioral Economics Strategies for Health Professionals
Sabem que majoritàriament els indicadors de salut dels catalans que empitjoren, tenen relació amb els comportament, amb els hàbits saludables. I que l'obesitat es troba al capdavant.
Entendre què cal fer és crucial. Però malauradament tenim visions i estratègies de curta volada. Ara acaba d'aparèixer un llibre que ofereix noves perspectives tot introduint l'economia del comportament davant el problema de l'obesitat. Diu:

Sabem que majoritàriament els indicadors de salut dels catalans que empitjoren, tenen relació amb els comportament, amb els hàbits saludables. I que l'obesitat es troba al capdavant.
Entendre què cal fer és crucial. Però malauradament tenim visions i estratègies de curta volada. Ara acaba d'aparèixer un llibre que ofereix noves perspectives tot introduint l'economia del comportament davant el problema de l'obesitat. Diu:
There are two ways of thinking about influencing behavior. The first is based on the standard rational model. That is, infl uencing what people consciously think about by increasing knowledge and awareness (known as the refl ective system ). This aproach assumes that the individual is a rational agent who surveys the situation to see what the various options are and then does a quick cost-benefi t analysis of those options in order to choose. The second approach is to alter the context within which people act (known as the automatic system ). This type of intervention is similar to the “nudge” outlined by Thaler and Sustein (2008), which often involves small changes to the choice environment. For example, one intervention tried to encourage school children to make healthier choices without alienating students by reducing their perceived choices. In a school cafeteria, what kids choose depends on the order in which the items are displayed.Els que llegiu aquest blog ja sabeu que m'hi he referit anteriorment en termes genèrics. Però aquest llibre esdevé més interessant perquè mostra amb molta precisió un canvi de perspectiva. Destaco una conclusió del primer capítol:
Rational food decisions often involve trade-off between short-term gains of sensory pleasure and longer term gains of health and wellness. Findings from behavioral economics research suggest that even when people are motivated to make healthy choices, external constraints in the decision-making process can prevent them from choosing optimally. Most of us prefer immediately gratifying short-term pleasure over our long-term goal of eating healthy. Errors in choices arise from systemic decision biases, emotion, and the limits of cognitive capacity.Atesa la importància de "l'epidèmia" potser caldria que més d'un hi fes una ullada. Encara que també vull anunciar que el capítol d'implicacions per a la política (el 12) és molt fluix. Us caldrà doncs una mica d'imaginació i reescriu-re'l vosaltres mateixos.

No us perdeu les friky-fotos de Diane Arbus al Jeu de Paume
(suggerit per un lector del blog i que em plau compartir amb valtros)
PS. Les retallades són notícia a la CNN, (confonen Catalunya amb Espanya, treball periodístic de nivell...)
09 d’abril 2015
Public Health Priorities
Start Well, Live Better: A Manifesto for the Public’s Health. London: UK Faculty of Public Health, 2014
These are the 12 suggested priorities for public health in UK for the next 5 years:
Give every child a good start in life

PS. Binge drinking 'costing UK taxpayers £4.9bn' Does anybody know how much does it cost here???
PS. In Spain, publicly funded health expenditure reached 64.150 million € in 2012,the amount for financial system bailout was 101.283 million € (p.24). Don't forget it: these are the priorities.
These are the 12 suggested priorities for public health in UK for the next 5 years:
Give every child a good start in life
- Give all babies the best possible start in life by implementing the recommendations of the 1001 Critical Days cross-party report
- Help children and young people develop essential life skills and make Personal, Social, Health and Economic, and Sex and Relationship Education a statutory duty in all schools
- Promote healthy, active lifestyles in children and young people by reinstating at least 2 h per week of physical activity in all schools
- Protect our children by stopping the marketing of foods high in sugar, salt and fat before the 9 pm watershed on TV, and tighten the regulations for online marketing
- Introduce a 20% duty on sugar-sweetened beverages as an important measure to tackle obesity and dental
- caries—particularly in children
- Tackle alcohol-related harm by introducing a minimum unit price for alcohol of at least 50 p per unit of alcohol sold
- Save lives through the rapid implementation of standardised tobacco packaging
- Set 20 m.p.h. as the maximum speed limit in built-up areas to cut road deaths and injuries, and reduce inequalities
- Enable people to achieve a good quality of life, health and wellbeing—give everyone in paid employment and training a ‘living wage’
- Reaffirm commitment to universal healthcare system, free at the point of use, funded by general taxation
- Invest in public transport and active transport to promote good health, and reduce our impact on climate change
- Implement a cross-national approach to meet climate change targets, including a rapid move to 100% renewables and a zero-carbon energy system

PS. Binge drinking 'costing UK taxpayers £4.9bn' Does anybody know how much does it cost here???
PS. In Spain, publicly funded health expenditure reached 64.150 million € in 2012,the amount for financial system bailout was 101.283 million € (p.24). Don't forget it: these are the priorities.
10 de desembre 2024
El peatge de l'obesitat
Economic impacts of overweight and obesity: current and future estimates for eight countries
Economic impacts of overweight andobesity: current and future estimates for161 countries
L'impacte econòmic de l'obesitat és d'un 2-3% del PIB, diuen en aquests articles, amb variacions importants:
The economic impact of OAO in 2019 is estimated at 2.19% of global gross domestic product (GDP) ranging on average from US$20 per capita in Africa to US$872 per capita in the Americas and from US$6 in low income countries to US$1110 in HICs
Aquests estudis consideren aquests costos:



i el cost total per aquí aprop equivaldria a un terç de la despesa sanitària pública que es fa en un any!

18 d’abril 2017
Exercise as a socially contagious activity
Exercise contagion in a global social network
Studies in social differences in health have a a new hurdle to tackle. How to boost social permeability? As Mackenback said in The Lancet on health inequalities: now it's personal.
PS. These are the results of the study in one figure:

Disciplines as diverse as economics, sociology, medicine, computer science, political science and physics have recently become interested in the interdependence of behaviours across the human social network. In particular, scientists have begun to ask whether our health and other behaviours are contagious, in that our decisions and actions affect the decisions and actions of our peers. If behavioural contagions exist, understanding how, when and to what extent they manifest in different behaviours will enable us to transition from independent intervention strategies to more effective interdependent interventions that incorporate individuals’ social contexts into their treatmentsA new study offers some of the first hard evidence that health-related habits can spread — and so perhaps could be deliberately seeded and encouraged — by social influence and peer pressure. Previous research has sought such a contagious effect in factors such as obesity and smoking, but the results have been inconclusive.
Studies in social differences in health have a a new hurdle to tackle. How to boost social permeability? As Mackenback said in The Lancet on health inequalities: now it's personal.
PS. These are the results of the study in one figure:
14 d’abril 2014
The Health of Catalans
La salut de la població de Catalunya en el context europeu
Comparing population health between countries allows to understand the scope of the differences. Some of them are unwarranted and others require an explanation. Anyway, it is good to confirm in a new report that the health of catalans has achieved a top level in Europe. The key indicator is healthy live years. As a summary it works, but when you go into details, then some problems arise: obesity, tobacco, colon cancer, diabetes,...
Comparing public expenditures , Catalonia spends less than other countries with similar GDP. And the opposite is true for private expenditures (p.16). Unfortunately, data is from 2010 and things have changed a lot, on GDP and health expenditure. My guess is that right now we are spending publicly a larger percentage than 6%. An update is needed in order to know better our current position.
Comparing population health between countries allows to understand the scope of the differences. Some of them are unwarranted and others require an explanation. Anyway, it is good to confirm in a new report that the health of catalans has achieved a top level in Europe. The key indicator is healthy live years. As a summary it works, but when you go into details, then some problems arise: obesity, tobacco, colon cancer, diabetes,...
Comparing public expenditures , Catalonia spends less than other countries with similar GDP. And the opposite is true for private expenditures (p.16). Unfortunately, data is from 2010 and things have changed a lot, on GDP and health expenditure. My guess is that right now we are spending publicly a larger percentage than 6%. An update is needed in order to know better our current position.
12 de maig 2021
Health behaviors and behavior change
Behavioral Economics and Public Health
Health behaviors and practices constitute the foundation of good physical and mental health. The leading contributors to the global burden of disease include tobacco smoking, low-quality diets, alcohol abuse, physical inactivity, and obesity. Accordingly, encouraging people to adopt—and maintain—healthy behaviors is a major objective of public health.
Today I recommend this book and this is what you'll find inside:
Chapter 1: An Introduction to Behavioral Economics and Public Health. Christina A. Roberto and Ichiro Kawachi
Chapter 2: Intertemporal Choices for Health. Justin S. White and William H. Dow
Chapter 3: Maintenance of Healthy Behaviors: Forming and Changing Habits. Dennis Rünger and Wendy Wood
Chapter 4: Emotions and Health Decision-Making: Extending the Appraisal Tendency Framework to Improve Health and Health Care. Rebecca Ferrer, William Klein, Jennifer Lerner, Valerie Reyna, and Dacher Keltner
Chapter 5: Social Norms, Beliefs, and Health. Brent McFerran
Chapter 6: Communicating for action: the importance of memorability and actionability. Jason Riis and Rebecca K. Ratner
Chapter 7:Nudging Individuals Toward Healthier Food Choices with the 4Ps Framework for Behavior Change. Zoë Chance, Ravi Dhar, Michelle Hatzis, and Kim Huskey
Chapter 8: Incentivizing Health Behaviors. Kristina Lewis and Jason Block
Chapter 9: Slim By Design: Moving from Can't to CAN.Brian Wansink
Chapter 10: Applying Behavioural Economics in a Health Policy Context: Dispatches from the front lines. Michael Sanders and Michael Hallsworth
Chapter 11: From Choice Architecture to Policy Infrastructure: Multi-Level Theory and the Political Economy of Health Behaviors. Frederick J. Zimmerman
14 de setembre 2019
On sugar and taxes
Should We Tax Sugar-Sweetened Beverages? An Overview of Theory and Evidence
The real question is how to tax the addiction industry. Sugar is only one case. Right now, these are the guiding principles (for sugar):

The real question is how to tax the addiction industry. Sugar is only one case. Right now, these are the guiding principles (for sugar):
1. Focus on Counteracting Externalities and Internalities, Not on Minimizing
Sugary Drink Consumption
2. Target Policies to Reduce Consumption among People Generating the Largest
Externalities and Internalities
3. Tax Grams of Sugar, Not Ounces of Liquid
4. Tax Diet Drinks and Fruit Juice If and Only If They Also Cause Uninternalized
Health Harms
5. When Judging Regressivity, Consider Internality Benefits, Not Just Who Pays the
Taxes
6. If Possible, Implement Taxes Statewide
7. The Benefits of Sugar-Sweetened Beverage Taxes Probably Exceed Their Costs
Furthermore, sugar-sweetened beverage taxes are not a panacea—they will not, by themselves, solve the obesity epidemic in America or elsewhere. But sin taxes have proven to be a feasible and effective policy instrument in other domains, and the evidence suggests that the benefits of sugar-sweetened beverage taxes likely exceed the costs
26 de maig 2017
Are You What You Eat?
Are You What You Eat? Healthy Behaviour and Risk Preferences
I am not strictly a fan of economic experiments. They are useful, but usually researchers achieve conclusions from samples and settings that are far from what happens really in population and geographies. However, some days ago I was looking at an article that it seemed of interest. They try to:
PS. Eliciting risk and time preference, the 2008 key article.
I am not strictly a fan of economic experiments. They are useful, but usually researchers achieve conclusions from samples and settings that are far from what happens really in population and geographies. However, some days ago I was looking at an article that it seemed of interest. They try to:
estimate the degree of risk aversion for a sample of young healthy adults and we explore its links with a broad range of risky behaviours considered together. Second, as indicator of the overall quality of diet, we complement, for the first time, the BMI with the Healthy Eating Index (HEI), and we relate both to estimated risk preferencesSounds good, because the use of Body Mass Index is absolutely outdated and its relationship with risk aversion is crucial. This is the summary:
Our results show that risk preferences significantly differ across young adults with different, not extreme, health conditions. In particular, they reinstate the importance of conducting analyses that look separately at the two sub-samples of female and male subjects . This allows disentangling the links and interactions between preferences and key health variables such as smoking, and also to fully account for the gender-specific effects of the BMI and of alternative indicators of healthy weight.
Second, in our sample young women do not show any significant robust associations between risk preferences and BMI. Third, for young men – but not women – the HEI index appears to be significantly and consistently associated with risk preferences: across all specifications, healthier nutritional habits, tend to be robustly associated with higher risk aversion. This, together with the lack of significance of BMI-based indexes, suggests that, for subjects with not extreme health conditions, there is a wide scope to use measures alternative (or complementary) to the BMI, as indicators of the overall quality of diet.That's it. And his final recommendation:
From a health policy perspective, our study suggests that in young adults who have not yet developed chronic or extreme health conditions, looking at a comprehensive nutritional indicator such as the HEI could provide more direct insights to the deeply rooted behavioural mechanisms that drive health behaviours than considering an indirect and increasingly questioned measure such as the BMI.Since children's obesity is one of the main challenges for health improvement, someone should take into account this message.
PS. Eliciting risk and time preference, the 2008 key article.
15 de gener 2021
Precision medicine
Precision Medicine for Investigators, Practitioners and Providers
Many topics under the same umbrella:
Table of Contents
Introduction
2. Role of genomics in precision medicine
3. High throughput omics in the precision medicine ecosystem
4. Infant gut microbiome
5. Paraprebiotics
6. Fecal transplantation in autoimmune disease
7. Drug pharmacomicrobiomics
8. CRISPR technology for genome editing
9. Engineering microbial living therapeutics
10. Organ on a chip
11. Multicellular in-vitro organ systems
12. The role of biobanks in biomarker development
13. Translational interest of immune profiling
14. Organoid pharmacotyping
15. Large datasets for genomic investigation
16. Modern applications of neurogenetics
17. Genomic profiling in cancer
18. Genomics in pediatrics
19. Genomics of gastric cancer
20. Genomics of prostate cancer
21. MicroRNAs and inflammation markers in obesity
22. MiRNA sequencing for myocardial infarction screening
23. Cell free DNA in hepatocellular carcinoma
24. Non coding RNA in cancer
25. Germline variants and childhood cancer
26. Pharmacogenomics in cancer
27. Proteomic biomarkers in vireoretinal disease
28. Proteomics in respiratory diseases
29. Cardiovascular proteomics
30. Host genetics, microbiome, and inflammatory bowel disease
31. Sampling, Analyzing, and Integrating Microbiome ‘omics Data in a Translational Clinical Setting
32. Omics and microbiome in sepsis
33. Molecular and omics methods for invasive candidiasis
34. Lipid metabolism in colorectal cancer
35. Salivary volatolome in breast cancer
36. immunodiagnosis in leprosy
37. decision support systems in breast cancer
38. Electronic medical records and diabetes phenotyping
39. Clinical signature of suicide risk
40. Machine learning and cluster analysis in critical care
41. Artificial intelligence in gastroenterology
42. Algorithms for epileptic seizure prediction
43. Precision medicine in ophthalmology
44. Phenotyping COPD
45. Lifestyle medicine
46. Precision medicine for a healthier world
47. Aging and clustering of functional brain networks
48. Nutrigenetics
49. Genome editing in reproductive medicine
50. MRI guided prostate biopsy
51. Precision Nutrition
52. Theranostics in precision oncology
53. Precision medicine in daily practice
54. Imaging in precision medicine
55. Organoid for drug screening
56. Printing of personalized medication using binder jetting 3D printer
57. 3 D printing in orthopedic trauma
58. Consumer genetic testing tools in depression
59. The future of wearables
60. Tumor heterogeneity and drug development
61. Smartphone based clinical diagnosis
62. Smartphone biosensing for point of care use
63. Data security and patient protection
64. Blockchain solutions for healthcare
65. Ethical questions in gene therapy
66. Pitfalls of organ on a chip technologies
67. Regulatory issues of artificial intelligence in radiology
68. Academic industrial alliance
69. The future of precision medicine
70. Precision Medicine Glossary
71. Useful internet sites

Subscriure's a:
Missatges (Atom)