
From: EU Statistics and book.
• By 2019 doctors who treat Medicare beneficiaries must choose between two options—enroll in a program called the merit-based incentive payment system or sign up to be part of an alternative payment model.Sounds interesting. Incentives and information altogether, a hint for other health insurance markets on what to do about it.
• The merit-based incentive payment system will adapt and combine multiple programs —PQRS, the EHR meaningful-use program, and the value-based payment modifier initiative—into one.
• Doctors opting for the merit-based incentive payment system must report quality-of-care measures to CMS. How is to be determined, but CMS likely will use an upgraded PQRS reporting system.
• Physicians will be scored on four components of care: quality (30 percent); resource
use (30 percent); meaningful use of EHRs (25 percent); and practice improvement activities (15 percent).
• Physicians choosing the alternative payment model path would have to be part of an integrated health system, join an ACO.

Theranos got a lot of traction by tapping into the frustration—both from consumers and the medical community—that diagnostic testing is too painful, too slow, and too expensive. “Their problem is they tried to do it with existing diagnostic instrumentation, instead of innovating new diagnostic instrumentation,”
Theranos is a black box that has touted results rather than process. “The ability of the lab medicine community to police and correct itself depends on that flow of information,” says Master. Instead, Theranos’ research was internal, and rather than submit their work to peer review the company cited their FDA approvals as evidence that the technology worked.At least in the USA there is a regulator, the FDA, lab regulation in Europe was enacted in 1998, completely outdated under a third party scheme, not a direct public regulator. Therefore, there is a pressing motive to speed up new and different rules in Europe. Microfluidics and nanotechnologies are calling for and urgent overhaul.
In 2005, Ms. Holmes hired Ian Gibbons, a British biochemist who had researched systems to handle and process tiny quantities of fluids. His collaboration with other Theranos scientists produced 23 patents, according to records filed with the U.S. Patent and Trademark Office. Ms. Holmes is listed as a co-inventor on 19 of the patents.
The patents show how Ms. Holmes’s original idea morphed into the company’s business model. But progress was slow. Dr. Gibbons “told me nothing was working,” says his widow, Rochelle. In May 2013, Dr. Gibbons committed suicide. Theranos’s Ms. King says the scientist “was frequently absent from work in the last years of his life, due to health and other problems.” Theranos disputes the claim that its technology was failing.

To more fully realize the benefits of behavioral insights and deliver better results at a lower cost for the American people, the Federal Government should design its policies and programs to reflect our best understanding of how people engage with, participate in, use, and respond to those policies and programs. By improving the effectiveness and efficiency of Government, behavioral science insights can support a range of national priorities, including helping workers to find better jobs; enabling Americans to lead longer, healthier lives; improving access to educational opportunities and support for success in school; and accelerating the transition to a low-carbon economy.Sounds interesting. It poses a tweak on the current approaches to policy design. Cass Sunstein says in NYT:
When government programs fail, it is often because public officials are clueless about how human beings think and act. Federal, state and local governments make it far too hard for small businesses, developers, farmers, veterans and poor people to get permits, licenses, training and economic assistance.
Behavioral research shows that efforts at simplification, or slight variations in wording, can make all the difference.The UK and now the USA are introducing this new way to define policies (and health policy). Let's keep an eye on its application and performance. What are we doing in this respect? Why are we waiting to introduce something similar?

The evidence shows that a wide range of preventive approaches are cost-effective, including interventions that address the environmental and social determinants of health, build resilience and promote healthy behaviours, as well as vaccination and screening. The evidence in this report shows that prevention is cost-effective in both the short and longer term. In addition, investing in públic health generates cost-effective health outcomes and can contribute to wider sustainability, with economic, social and environmental benefits.Cost-effectiveness studies are usually focused towards treatments. This report shows some examples related to public health. Unfortunately, this is not so common. Up to now my reference on this tòpic was this article. Now I'm adding this report by WHO Euro. And the question remains: if these interventions are so cost-effective, why are we waiting for their implementation?
It is recognized that a comprehensive strategy needs to include a combination of population and targeted individual preventive approaches, but it should be noted that, on average, individual-level approaches were found to cost five times more than interventions at the population level (WHO, 2011a). In general, evidence also shows that investing in upstream population-based prevention is more effective at reducing Health inequalities than more downstream prevention (Orton et al., 2011). Meanwhile, the National Institute for Health and Care Excellence in the United Kingdom found thatmany public health interventions were a lot more cost-effective than clinical interventions (using cost per QALY), and many were even cost-saving (Kelly, 2012).
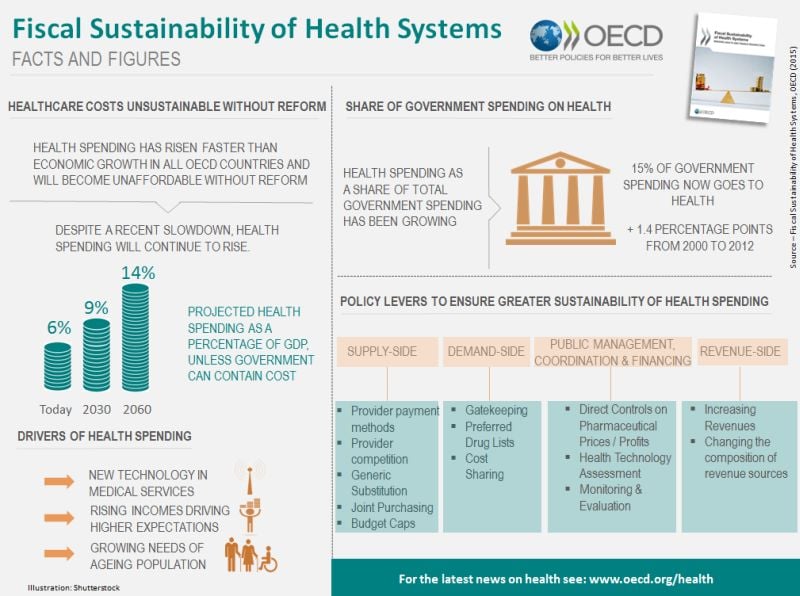
The OECD defines fiscal sustainability as the ability of a government to maintain public finances at a credible and serviceable position over the long term (OECD, 2013). Fiscal sustainability implies governments are able to maintain policies and expenditure into the future, without major adjustments and excessive debt burdens for future generations. The term refers to overall government spending, revenues, assets and liabilities that reflect past commitments and adapt to future trends such as socio-economic trends and environmental factors.
For the health sector, fiscal sustainability is perhaps best understood as a constraint that needs to be respected, rather than an objective in itself (Thomson et al., 2009). This implies that how governments achieve fiscal sustainability matters, rather than it becoming a simple cost-cutting exercise.Of course!. Sometimes OECD writes obvious statements. There is a budget constraint! Perhaps someone has forgotten it.
Gains in health since 1970 for the causes analysed in this chapter have clearly been enormous. While not all of these declines can be attributed to health policies, part of the decline in all these causes can be, as shown in the previous chapters. For example, some of the declines in lung cancer and ischaemic heart disease can be attributed to tobacco control; some of the declines in external cause mortality among children to injury prevention, and some of the declines in death rate from RTIs to road safety measures, and so on. It is impossible to estimate the specific contribution of preventive health policies to these declines, but even if these accounted for only half or a quarter of the cause-specifi c declines, the successes would be immense. At the same time, not all countries have been equally successful in bringing down mortality from these preventable causes, as shown again by the calculations.