Deirdre McCloskey presenting "How the World Grew Rich: The Liberal Idea, Not Accumulation or Exploitation" at Nobel Conference, Sept 29, 2016
PS. Quote of the day:_
What is crucial is our ability to engage in continuous conversation, testing one another, discovering our hidden presuppositions, changing our minds because we have listened to the voices of our fellows. Lunatics also change their minds, but their minds change with the tides of the moon and not because they have listened, really listened, to their friends' questions and objections.
A.O. Rorty, "Experiments in Philosophical Genre: Descartes' Meditations," pp. 545-565 in Critical Inquiry 9: 562
This is the great question that Deirdre Nansen McCloskey tries to answer in her last book of the trilogy. If we want to continue to improve our living standards we should confirm that we are on the right track. And she says:
"an anti-bourgeois rhetoric, specially if combined with the logic of vested interests, has in many ocasions damaged societies"
She focuses specially on how specific places changed their views on those that create value. Part IV explains how a pro-bourgeois rhetoric was formed in England around 1700:
In other words, the attitude of medieval Europe and its church toward the bourgeoisie was nothing like entirely hostile, especially in northern Italy and in some of the ports of Iberia and the Baltic, even if it did not result in the business-dominated civilization of the southern Low Countries after 1400, and more widely Holland after 1568, and England after 1688. Barcelona, for example, was from medieval times an exception to the antibourgeois character of the rest of Spain—as in some ways it still is, and as Basque Bilbao came to be in the nineteenth century
Realizing the potential depended on a bourgeois ideology adopted by whole societies, not merely by the bourgeoisie itself. The ideology had been foreshadowed in the Hanse towns such as Lübeck and Bergen and Danzig, and in some trading towns of southern Germany, and in the prosperous little cities of Flanders and Brabant, in Barcelona, in the Huguenot strongholds of France, and especially in the northern Italian cities such as Venice, Florence, Genoa, and the rest.
In summary, a change in ideas modified deeply wealth creation. I can't summarise 768 pages. My recommendation is to read it if you are interested in economic history. The key questions are answered there and in two previous books. You may agree or not, but persuasive style of Mccloskey is guaranteed. Some parts are repetitive and controversial, but the amount of quotes and knowledge is amazing. You'll enjoy the impressive erudition of Deirdre McCloskey.
PS. Today in the news has started a new anti-bourgeois campaign, the goal is to increase the taxes of the super-rich. It just sounds really as the opposite of what Deirdre says that has allowed us the betterment process of the last three centuries. Our economics minister is professor of economic history. It would be good that somebody gifts him the book and convinces him to read it.
PS. While I was studying my PhD, in rhetorics course, Deirdre came. I will always remember how she argued about the need to change economic methodology. Unfortunately after two decades, the academic profession has taken the opposite direction, a mathematical perspective.
PS. Eduard Bonet, from ESADE, is quoted several times in the book. I would like to acknowledge his guidance on this topic.
Unfortunately the US government has discontinued the Healthcare Horizon Scanning System. It was a framework to detect innovations before entering into the market. One of the last reports was on cost impact of these technologies:
We completed 53 rapid cost analyses on 55 topics over a period of 4 months from July through November 2014. The topics consisted of selected Potential High Impact ntervention reports published in 2013 and 2014. These 55 topics had a designation of oderate or high potential for high impact in those reports. To estimate potential costs of these new and emerging interventions, we sought to identify data on the following: revalence of the disease or condition targeted by each intervention; actual or projected doption of the new intervention; costs of the intervention; costs of a similar intervention; and costs of an alternative intervention used for the disease or condition
It seems that something similar is being proposed in Europe. Let's wait and see. Meanwhile check the canadians.
The topic sould be at the top of health policy agenda (at least as it is in this blog). New evidence confirms the additional safety risks of european bad regulation.
In the European Union, medical devices are approved by private notified bodies if they meet performance criteria and are likely to be safe, but notified bodies generally do not require evidence of effectiveness for most devices. Many high risk devices are approved faster in the EU than in the United States, where the Food and Drug Administration usually requires prospective clinical trials of such devices.
The unadjusted rate of safety alerts and recalls for devices approved first in the EU was 27% (62/232) compared with 14% (11/77) for devices approved first in the US. The adjusted hazard ratio for safety alerts and recalls was 2.9 (95% confidence interval 1.4 to 6.2) for devices approved first in the EU.
This means exactly 2.9-fold greater rate of safety alerts and recalls and a 4.6-fold greater rate of recalls than devices approved first in the US (and if you look at the confidence intervals you'll get more worried). How can we trust the european regulator?. For decades, European Union has leaved its citizens with less safety protection than is required for medical devices. A perfectly designed absurdity to disseminate risk for european citizens that the new proposed regulation is unable to correct.
PS. If you wnat to understand the differences between EU and US regulation, read this NEJM article or Milbank one..
If you want to know if some device is effective, there is a standard way to demonstrate it: a clinical trial. This is precisely what has been done on the impact of wearables on weight loss. And the result is:
Among young adults with a BMI between 25 and less than 40, the
addition of a wearable technology device to a standard behavioral
intervention resulted in less weight loss over 24 months. Devices that
monitor and provide feedback on physical activity may not offer an
advantage over standard behavioral weight loss approaches.
That's amazing! Why is there so many articles pushing wearables for weigth loss when there are very few clinical trials, and their results are clearly against their use?. This is a marketing bubble and somebody should tell clearly that they could use wearables but for other reasons.
PS. Let's imagine that somebody wants to relate wearables for weight loss reduction with insurance premiums! Nothing to add.
If there is an example of how one part of an organization can't speak with the other is the European Union and Health Policy. If we are talking about medical devices, health issues are at the back, industry is writing the regulations. If we are talking about options for improvement, economics unit explains what health unit has to do. A perfectly designed mess.
Take the example of this week. A Joint report, that is an economics report with elementary mistakes for any health economist. Take this statement:
"Competition between hospital providers can lead to higher quality under strict price regulation." (p.70)
Does anybody know what does really mean strict regulation? Who is writing such things and being paid with our taxes?.
If you check another report on the topic by experts of the European Union you'll find an opposite recomendation.
"The conditions for competition to be a useful instrument vary across countries, health care subsectors and time. There is no golden rule or unique set of conditions that can be met to ensure that competition will always improve the attainment of health system goals." (p.4)
Definitely, the EU is in the middle of no judicious health policy.
In summary, an avoidable report that you can skip reading and devote your time to hearing Bob Dylan music for example, the new Nobel Prize.
Come gather 'round people where ever you roam
And admit that the waters around you have grown
And accept it that soon you'll be drenched to the bone
If your time to you is worth savin'
Then you better start swimmin' or you'll sink like a stone,
For the times they are a' changin'!
Come writers and critics who prophesy with your pen
And keep your eyes wide the chance won't come again
And don't speak too soon for the wheel's still in spin
And there's no tellin' who that it's namin'
For the loser now will be later to win
For the times they are a' changin'!
Come senators, congressmen please heed the call
Don't stand in the doorway don't block up the hall
For he that gets hurt will be he who has stalled
There's a battle outside and it's ragin'
It'll soon shake your windows and rattle your walls
For the times they are a' changin'!
Come mothers and fathers throughout the land
And don't criticize what you can't understand
Your sons and your daughters are beyond your command
Your old road is rapidly agin'
Please get out of the new one if you can't lend your hand
For the times they are a' changin'!
The line it is drawn the curse it is cast
The slow one now will later be fast
As the present now will later be past
The order is rapidly fadin'
And the first one now will later be last
For the times they are a' changin'!
After all these years, a new proposal for regulating in vitro diagnostics and medical devices in EU is available. Current regulation was enacted in 1998, and this one could be applicable in 2022, 24 years after, pas mal for the busy politicians!.
And this is a proposal, there were previous unapproved proposals, and this one has to pass the Council and the Parliament. I will not enter into the details.
It was supposed to increase safety and efficacy, but the main problem remains with who has to enforce them. Notified bodies, a subcontracting regulatory firms network, with vested interests with industry can't claim independence. And specifically, the methods for evaluate the analytical validity, clinical validity and utility is uncertain. No regulator will confirm us that the cut-off values of diagnostic tests are set according to the best evidence and greatest benefit. In US, FDA is the responsible.
In summary, a new missed opportunity for european citizens. A greater risk and uncertain effectiveness in diagnostic tests and medical devices.
PS. The latest known example of the impact of wrong regulation is this one. Those affected can't read this blog, they are blind.
Cost-effectiveness may be considered a focal point for health economists. However the trip from theory to implementation raises many doubts. The reductionist perspectives of some health economists consider that politicians are rational in decision making. And this is not the case. I suggest you a look at this article:
The cost-effectiveness model generally used for the evaluation of health technologies—and health care and public health interventions more widely—has become a central tool for public-sector policy makers in many health care systems. It was developed to help decision makers with fixed public resources to compare (1) different interventions for the same health problem and (2) programs in different disease areas. For a particular level of health care resources, the goal is to
choose from among all possible combination of programs the set that maximizes total health benefits produced. The traditional CEA methods presume the existence of only one salient constraint— the public finance budget constraint. Yet all of the evidence suggests that many other constraints impinge on decision makers, at least in the short run.
A fundamental reason for the failure to implement is that CEA assumes a single constraint, in the form of the budget constraint, whereas in reality decision makers may be faced with numerous other constraints. The objective of this article is to develop a typology of constraints that may act as barriers to implementation of cost-effectiveness recommendations. Six categories of constraints are considered: the design of the health system; costs of implementing change; system interactions between interventions; uncertainty in estimates of costs and benefits; weak governance; and political constraints.
There is intelligent life beyond cost-effectiveness...
All what you need to know about the implications of stratified medicine, you can get it in one article. That's great. And at the same time worrying or amazing for somebody. You'll see that stratified medicine reduces the size of the market with the use of biomarkers. Than, more accuracy is more costly. However, who sets the cut-off? This is the question. Trusheim and Berndt shed light on the issue:
Setting the cut-off value for the imperfectly performing companion diagnostic presents multiple challenges to the scientist, regulator, ethicist, marketer, clinician, and payer. Scientists might seek natural break points connected to a biological mechanistic rationale, or struggle to define the proper balance between diagnostic sensitivity and specificity. Regulators might seek a division that maximizes the benefit:risk ratio with the greatest certainty. Ethicists might be concerned with issues of denying care to some or knowingly causing harm to some (statistically) to benefit others. Marketers might seek to optimize revenues by balancing efficacy improvements, and the correlated pricing and market share, with the number of eligible patients in the market. Clinicians might seek to know the likelihood that their individual patient will respond to treatment or will incur an adverse event. Payers might focus on the net clinical benefit to their specifically covered population and the overall affordability of the resulting net total outlays for the actually treated population. Although clearly having overlapping perspectives, when selecting the CDx cut-off each stakeholder brings its own unique view of the issues to emphasize and the proper metrics to optimize.
Meanwhile, you'll not be able to find any implication of the regulator on selecting the right cut-off in the new european draft rules for in vitro diagnostic tests. This is a new missed chance.
Today I'll suggest a reading from the latest issue of Nota d'Economia. You'll find two articles of special interest for health economists. The first one, on institutional design will convince you that this is the tough part of the issue. Governments prefer to avoid difficult decisions, only a proper institucional design will provide the best impact of economic evaluation. The second one is an excellent example of the impact of stroke prevention and care, or how organizational innovation may deliver social value of 372M€ in 7 years. Great, we need more initiatives like that, and studies that assess its impact.
This is the summary:
Aquest estudi mostra que després de les millores que han tingut lloc en l’atenció a l’ictus agut a Catalunya (Abilleira et al., 2009, 2011a, 2011b; Salvat-Plana et al., 2011) en el període 2005-2012 es van evitar 719 defuncions i es van guanyar 11.153 anys de vida, amb un valor social mínim de 353.164.622,08 euros (1.050.147.483,07 euros màxim). Un cop eliminat l’efecte de l’augment de la incidència, el nombre de defuncions per ictus va ser de 919 i 11.760 anys de vida guanyats, amb un valor social mínim de 372.404.624,76 euros (1.195.167.115,79 màxim)
PS. US is affraid of economic evaluation...have a look at JAMA
What happens if "one quarter of the clinical genetic results from commercially available multiplex cancer panels and reported at the PROMPT registry had conflicting interpretations" and if "36% of conflicting genetic tests results appeared to be clinically relevant, because they were either reported as pathogenic/likely pathogenic"? Does anybody care about it?.
I would suggest today you have a look at this article and your level of anxiety will increase suddenly.
Clinical data and genetic testing results were gathered from1,191 individuals tested for inherited cancer susceptibility and self-enrolled in PROMPT between September 2014 and October 2015. Overall,participants (603 genetic variants) had a result interpreted by more than one laboratory, including at least one submitted to ClinVar, and these were used as the final cohort for the current analysis.
Of the 603 variants, 221 (37%) were classified as a variant of uncertain significance (VUS), 191 (32%) as pathogenic, and 34 (6%) as benign. The interpretation differed among reporting laboratories for 155 (26%). Conflicting interpretations were most frequently reported for CHEK2 and ATM, followed by RAD51C, PALB2, BARD1, NBN, and BRIP1. Among all participants, 56 of 518 (11%) had a variant with conflicting interpretations ranging from pathogenic/likely pathogenic to VUS, a discrepancy that may alter medical management.
Therefore,
Clinical interpretation of genetic testing for increased cancer susceptibility as assessed by multiplex panels hinges on accurate curation and interpretation of variants. Discrepant interpretation of some genetic variants appears to be common.
Take care. The regulator remains on vacation, a never ending vacation.
Diagnostic tests show
different levels of false positive and negatives in the results. The
impact of such unwanted results by physicians finally have an impact on
health and quality of life of patients. You can check what does this
means for HER-2 test in breast cancer in US in this article.
Patients
with breast cancer whose tumors test positive for human epidermal
growth factor receptor 2 (HER2) are treated with HER2-targeted therapies
such as trastuzumab, but limitations with HER2 testing may lead to
false-positive (FP) or false-negative (FN) results.
Among 226,870
women diagnosed with EBC in 2012, 3.12% (n = 7,070) and 2.18% (n =
4,955) were estimated to have had FP and FN test results, respectively.
Approximately 8400 QALYs (discounted, lifetime) were lost among women
not receiving trastuzumab because of FN results. The estimated
incremental per-patient lifetime burden of FP or FN results was $58,900
and $116,000, respectively. The implied incremental losses to society
were $417 million and $575 million, respectively.
Absolute
certainty in diagnosis is unattainable, no matter how much information
we gather, how many observations we make, or how many tests we perform. A
diagnosis is a hypothesis about the nature of a patient's illness, one
that is derived from observations by the use of inference. Our task is
not to attain certainty, but rather to reduce the level of diagnostic
uncertainty enough to make optimal therapeutic decisions.
USA is well known for its prominent interest in avoiding cost-effectiveness as we know in certain european countries. They talk about comparative effectiveness research, because it fits with their current priorities: What works best? and let's the cost for another day. Forget trade-offs.
If you want to know the recent stuff on the topic, have a look at this article. You'll notice three steps: clinical care value, managing affordability and health system value. It makes sense as a first step. In our country we don't have such official estimates. The next step should be to introduce cost and equity considerations.
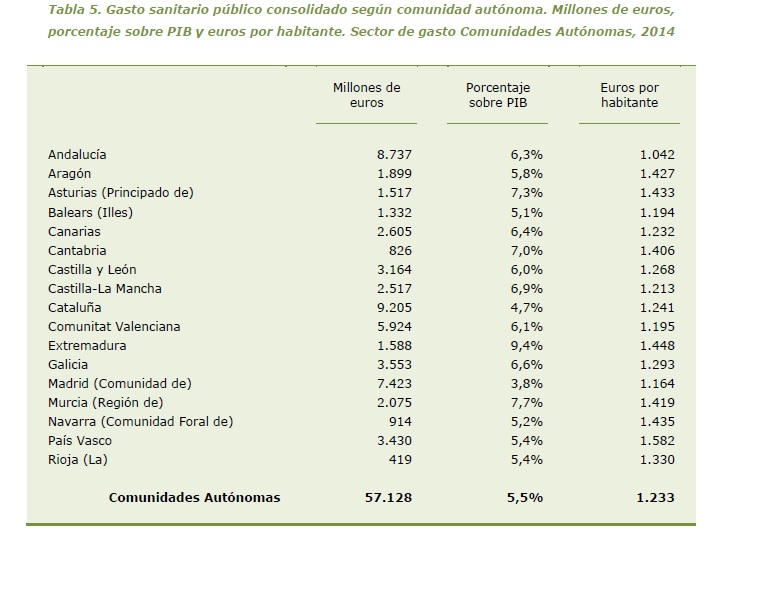
Let's imagine an alleged State. All its citizens pay taxes under the same Tax Code. Health Benefits are the same under the Health Act. And spending on health care according to geography, can reach 52% more in Basque country compared to Andalusia. This is not new. Many decades having the same figure and nobody cares about it.
This is an easy table to understand health policy making in a failed state. Catalonia spends 4,7% of GDP on health, other sources say 5,5%. Anyway, you'll not find an OECD country with similar figures. After a decade we are spending the same amount per citizen than in 2006, 1.120 €. I will not add anything to this mess. There is only an increasing need to disconnect. Is there any MP in the room?
PS. I'm not arguing that every country has to spend the same, I'm just saying that it is not legally possible to deliver the same benefits with such different budgets. Therefore we are unequal before law. This is the usual legal uncertainty of a failed state.
JAMA has decided to start JAMA Professionalism, a new department.
The goal of the articles in this section is to help physicians fulfill required competencies on this topic. According to the American Board of Medical Specialties definition, professionalism is “…a commitment to carrying out professional responsibilities, adherence to ethical principles and sensitivity to diverse patient populations.” Taking responsibility for executing professional responsibility seems intuitive enough. But what does it mean to adhere to ethical principles? How are the ethical principles defined?
Good questions. And the answers for US physicians are in the new AMA Code of Medical Ethics.
A multi-year effort to modernise that has provided an interesting outcome. You can check for example, regarding prioritisation of resources, what should be done? in chapter 11 you'll find the answers. A good suggestion for our physicians' associations and their outdated codes.
How do you want to manage, with a rearview mirror or just looking forward? Big data allows to look forward with better precision. The uncertainty about the disease and about the cost of care is large when you enter in hospital from an emergency department. But, after the diagnosis (morbidity), could we estimate how much could cost an episode?. If so, then we could compare the expected cost and the observed cost on a continous process.
Right now this is possible. Check this article that we have just published and you'll understand that costs of different services according to morbidity can be reckoned and introduced in health management. This analysis goes beyong our former article, much more general. So, what are we waiting for? Big data is knocking at the door of health care management, predictive modeling is the tool.
Amazing concert by Caravan Palace in Sant Feliu de Guixols three weeks ago.
While reading today FM Alvaro op-ed on current war: Questions in a war, I thought that was good to remember Jack Hirshleifer and specifically to retrieve an excellent speech he gave in 1993: The dark side of the force. When I read it for the first time I got impressed and I've remembered forever.
Therefore, my suggestion is to read the whole speech. If you are an economist, you'll be shaken by his views. Selected statements:
“Our profession has on the whole taken not too harsh but rather too benign a view of the human enterprise. Recognizing the force of self-interest, the mainline Marshallian tradition has nevertheless almost entirely overlooked what I will call the dark side of the force—to wit, crime, war, and politics."
“cooperation, with a few obvious exceptions, occurs only in the shadow of conflict.” “when people cooperate, it is generally a conspiracy for aggression against others (or, at least, is a response to such aggression).”
"Pareto is saying, sure, you can produce goods for the purpose of mutually beneficial exchange with other parties—OK, that's Marshall's "ordinary business." But there's another way to get rich: you can grab goods that someone else has produced. Appropriating, grabbing, confiscating what you want— and, on the flip side, defending, protecting, sequestering what you already have—that's economic activity too. Take television. Cops chase robbers, victims are stalked by hitmen (or should I say hitpersons?), posses cut off rustlers at the pass, plaintiffs sue defendants, exorcists cast spells against vampires. What is all this but muscular economics? Robbers, rustlers, hitpersons, litigants—they're all trying to make a living. Even vampires are making economic choices: sucking blood is presumably the cost-effective way of meeting their unusual nutritional needs.”
“This is Machiavelli's version of the golden rule: he who gets to rule, will get the gold. Human history is a record of the tension between the way of Niccolo Machiavelli and what might be called the way of Ronald Coase. According to Coase's Theorem, people will never pass up an opportunity to cooperate by means of mutually advantageous exchange. What might be called Machiavelli’s Theorem states that no one will ever pass up an opportunity to gain a one-sided advantage by exploiting another party.
Machiavelli's Theorem standing alone is only a partial truth, but so is Coase's Theorem standing alone. Our textbooks need to deal with both modes of economic activity. They should be saying that decision-makers will strike an optimal balance between the way of Coase and the way of Machiavelli—between the way of production combined with mutually advantageous exchange, and the dark-side way of confiscation, exploitation, and conflict.”
"Thus, in recognizing the role of conflict we must not go overboard in the other direction. All aspects of human life are responses not to conflict alone, but to the interaction of the two great life-strategy options: on the one hand production and exchange, on the other hand appropriation and defense against appropriation. Economics has done a great job in dealing with the way of Ronald Coase; what we need now is an equally subtle and structured analysis of the dark side: the way of Niccolo Machiavelli.”
The balance between these modes of economic activity--the one leading to greater aggregate wealth, and the other to conflict over who gets the wealth--provides the main story line of human history.
This speech and several articles on conflict were published in a book "The Dark Side of the Force: Economic Foundations of Conflict Theory".
Hirshleifer analytic frame may be applied to health economics as well, specifically to such cases where fraud, inappropriateness, and false advertising are part of the dark force.
PS. Long time ago I quoted in a post the Schelling book on the same topic.
A new milestone has been achieved in Medicine. Tracking epigenetic alterations is crucial to understand a disease. However, epigenetic biomarkers are needed to assess such changes. Its precision (sensitivity-specifity) is paramount for its clinical application. Now a group of international researchers has certified its performance (partially). Have a look at this Nature article:
Genome-wide mapping and analysis of DNA methylation has become feasible for patient cohorts with thousands of samples, and epigenome-wide association studies have been conducted for numerous biomedically relevant phenotypes. To translate relevant epigenome associations into clinically useful biomarkers, it is necessary to select a manageable set of highly informative genomic regions, to target these loci with DNA methylation assays that are sufficiently fast, cheap, robust and widely available to be useful for routine clinical diagnostics, and to confirm their predictive value in large validation cohorts.
Among its conclusions I would like to highlight three of them:
(i) Absolute DNA methylation assays are the method of choice when validating DNA methylation differences in large cohorts, and they are also an excellent technology for developing epigenetic biomarkers.
(ii) Relative DNA methylation assays are not a good replacement for absolute assays. However, experiences of scientists in the contributing laboratories suggest that carefully selected, designed and validated relative assays can cost-effectively detect minimal races of methylated DNA against an excess of unmethylated DNA.
(iii) Global DNA methylation assays suffer from noisy data and divergent results between technologies. Locus-specific assays (possibly combined with prediction) provide a more robust alternative
That's it. Very soon will see the epigenetic biomarkers in routine clinical use. And afterwards, epigenetic drugs and treatments. Then, we'll confirm that the promise of precision medicine is a reality. The implications for medicine as a scientific discipline and clinical decision making are huge, and specifically, healthcare organizations will need to adapt to new knowledge and technologies.
This is the main message of the book: Do not send generic messages on food and its risks, the time for segmentation has arrived,
A generic approach, involving the provision of vast amounts of information to the general public, stands a real risk of leading to information overload, bewilderment and lack of interest among mainstream consumers. A more effective approach to change consumer food buying and consumption behaviour, is to focus on segmenting the population according to their information needs, and developing information with high levels of personal relevance to specific groups of respondents who may be at greater risk than the rest of the population. Such information is more likely to create attitudinal change and subsequent behavioural change as the perceived personal relevance is high.
A long time has passed since WHO published a book on voluntary health insurance, just a decade (!). Therefore, there are many reasons to review again what's going on, and this is precisely what you'll find in two recent books.
Before any recommendation, it is good to have a good analysis. And the best analysis comes from reliable data. Somebody should check the published data in the book. In the case of Spain it says 10% of suplementary insurance, while it is around 16% (!) (p.50) (and it is duplicate really according to OECD classfication). And beyond that, it says that there is 3% of voluntary health insurance that is substitutive, while it is exactly 0% (!). Therefore take care. I'll not comment anything else.
The Lancet has just published a new estimate of the size of health expenditures in the future up to 2040. Too often nobody looks backward and check what predictions said before. If somebody does it, it will get a surprise for the first time, however the following ones he will convey that predictions are useless, because there are too many uncertain situations to take into account. Basically most of the hypothesis are flawed. Take this statement from the article:
Despite remarkable health gains, past health fnancing trends and relationships suggest that many low-income and lower-middle-income countries will not meet internationally set health spending targets and that spending gaps between low-income and high-income countries are unlikely to narrow unless substantive policy interventions occur. Although gains in health system efficiency can be used to make progress, current trends suggest that meaningful increases in health system resources will require concerted action.
Is there anybody that can tell me what "internationally set health spending targets" are?. Who sets them?. If anybody wants to check what I'm saying, have a look at the cutbacks from the great recession and the estimates by OECD or EU. Everybody was saying that technology innovation and aging would boost health expenditures forever, and now we know that this is not true. Forget the article. Distrust the fortune-tellers.
Last month I was saying that business strategy à la Porter required a new perspective, the platform view. Beyond that, blockchain represents a potential disruption of current business and information and communication technologies as of today.
My suggestion is to have a look at the crucial book by Mougayar on The Business Blockchain. You'll get a clear understanding that a deep transformation is in process.
How to think holistically about the blockchain as a meta technology, a business model disruptor, and legal/regulatory policies challenger.
The 10 properties exhibited by the blockchain (beyond its most popular one, as a distributed ledger)
Blockchains as a new Internet layer, comprised of the new breed of decentralized applications.
The unbundling of trust and how a new form of trust inserts itself between peer-to-peer relationships, and brings a new level of transparency, trust and truth.
The rise of New Intermediaries. Just as the Internet replaced some intermediaries, now the blockchain is replacing other intermediaries, while simultaneously creating new ones.
Industry cases in healthcare, energy and government, including an in-depth review of financial services.
Practical recommendations for implementing the blockchain within the enterprise.
The blockchain as the operating system that enables decentralization, and its technological, political and societal implications.
The birth of a crypto economy that creates its own wealth via new business models, and peer-to-peer transactional relationships between producers and consumers.
A new flow of value, with the blockchain acting as the digital leveler that moves value across a new variety of markets.
47 blockchain predictions about a not-so-distant future, when blockchain technology permeates our world and creates new companies and new services.
Promising contributions to healthcare:
The theory is attractive: publish your medical record safely on the blockchain and be assured that you or an authorized person can access it anywhere in the world. That is what the governmentof Estonia has done—a good case of blockchain technology in healthcare. Using Guardtime’s large scale keyless data authentication, in combination with a distributed ledger, citizens carry their ID credentials which unlock access to their healthcare records in real-time. From that point forward, the blockchain ensures a clear chain of custody, and it keeps a register of anyone who touches these records, while ensuring that compliance process is maintained.
Other healthcare usages might include:
Using a combination of multisignature processes and QR codes, we can grant specific access of our medical record or parts of it, to authorized healthcare providers.
Sharing our patient data in the aggregate, while anonymizing it to ensure privacy is maintained. This is helpful in research, and for comparing similar cases against one another.
Recording and time-stamping delivery of medical procedures or events, in order to reduce insurance fraud, facilitate compliance and verification of services being rendered.
Recording the maintenance history of critical pieces of medical equipment, for example, an MRI scanner, providing a permanent audit trail.
Carrying a secure wallet with our full electronic medical record in it, or our stored DNA, and allowing its access, in case of emergency.
Verifying provenance on medications, to eliminate illegal drug manufacturing.
“CaseCoins:” originating specific altcoins that create a cryptocurrency market around solving a particular disease, such as FoldingCoin, a project where participants share their processing power to help cure a disease, and get rewarded with a token asset.
Definitely, this is a key book to understand blockchain and again, there is room for healthcare. Wether the promise will become a reality, it's uncertain today.
Blockchain, the technology behind bitcoin, the virtual currency, could be the new tool that could change the current state of health records and healthcare information. Up to now we have been discussing about interoperability between systems. What would happen if the citizen is the owner of the information and he has all data available everywhere anytime?. This is what certain initiatives try to define right now. Something like this initiated by the physician would be the data owned by the patient:
We are at the begining of a great transformation. I don't now if the appropriate word is revolution. Anyway, if you are interested in the topic you may check som details here.
However if you want a deep review of whats going on in 12 critical disruptions, read chapter 6 of the book "Blockchain revolution". You'll find there the potential impact on health:
In the health care sector, professionals use digitization to manage assets and medical records, keep inventory, and handle ordering and payments for all equipment and pharmaceuticals. Today, hospitals are full of smart devices that oversee these services, but few communicate with one another or take into account the importance of privacy protection and security in direct patient care. Blockchain-enabled IoT can use emerging applications to link these services. Applications in development include monitoring and disease management (e.g., smart pills, wearable devices to track vital signs and provide feedback) and improved quality control. Imagine an artificial hip or knee that monitors itself, sends anonymized performance data to the manufacturer for design improvements, and communicates with a patient’s physician, “Time to replace me.” Technicians will be unable to use specialized equipment if they haven’t taken prerequisite steps to ensure their reliability and accuracy. New smart drugs could track themselves in clinical trials and present evidence of their effectiveness and side effects without risk of modified results.
If you are interested in innovation and want to follow the next wave, the internet of value, then you need to read such book. Definitely, there is wide room for health in blockchain.
The book on "Wisdom of crowds" became popular claiming that the aggregation of information in groups achieved decisions that are often better than could have been made by any single member of the group. Now in Medical Decision Making you'll find an article that applies such reasoning to clinicians. And it says:
Little research has been done on whether the average of clinicians making predictions is more accurate than the individual clinicians themselves or whether their average prediction compared favorably to statistical predictions. The purpose of the present study is to examine the predictive accuracy of the average of individual clinician predictions and to compare this average to the accuracies of individual clinicians and to a published statistical model.
And the four conclusions are:
First, it would appear that the averages of the clinicians perform better than clinicians individually. All the clinicians on their own performed with a concordance index of 0.628. However, averaging the predictions of just a pair of clinicians had better performance. Second, the performance tends to improve as more clinician predictions are averaged. Interestingly, at least in this study of a limited number of clinicians, although performance was seen to continually improve as clinicians were added, there was decreasing marginal return for increasing group sizes. Third, as the group size increased (see Figure 2), the performance of the averaged clinicians approached that of the best individual clinician (from Figure 1), suggesting that much larger clinician groups are needed for the performance of the average to be better than that of the best clinician. And fourth, even averaging all of the clinicians’ predictions was inferior to that of the statistical model.
The authors recognise their study limitations, however some insights are useful to take into account. Let's ponder on how many "second opinions" would be approppriate.
This Wednesday at Saló del Tinell in Barcelona, great concert by Capella de Ministrers on Ramon Llull,the last pilgrimage
Once again, we do need a comprehensive definition of what is health and wellbeing, and the current issue of PNAS provides us with an interesting approach:
The dominant model of health is a disease-centered Medical Model (MM), which actively ignores many relevant domains. In contrast to the MM, we approach this issue through a Comprehensive Model (CM) of health consistent with the WHO definition, giving statistically equal consideration to multiple health domains, including medical, physical, psychological, functional, and sensory measures. We apply a data-driven latent class analysis (LCA) to model 54 specific health variables from the National Social Life, Health, and Aging Project (NSHAP), a nationally representative sample of US community-dwelling older adults.
Although public health campaigns, such as “Choosing Wisely,” rightly emphasize the need to decrease unnecessary health interventions (52), they still accept the basic health conception of the MM as resting on organ system disease. Instead, the CM instantiates comorbidities and the equal importance of mental health, mobility, and sensory function in health and should inform policy redesign. For example, including assessments of sensory function, mental health, broken bones in middle age, and frailty in annual physician visits would enhance risk management. In addition to policies focused on reducing BMI, greater support for preventing loneliness among isolated older adults would be effective. In place of additional (expensive) new medicines for hypertension, helping older adults find social support through home care services or alternative living arrangements could be developed. In summary, taking a broad definition of health seriously and empirically identifying specific constellations of health and comorbidities in the US population provide a new way of assessing health and risk in older adults living in their homes and thereby, may ultimately inform health policy.
And these are the results:
The CM of health with six distinct health classes based on 54 health measures across six dimensions (listed in column 1). The column US population (US Pop.) reports the prevalence in 2005 of each disease or condition in the older US Pop. ages 57–85 y old (definitions and validation are in Fig. S1). Within each health class (columns), the prevalence of a given disease or condition indexes the likelihood that any member of the class has that particular disease [rows; n = 54 health measures ordered by prevalence within each health domain (column 2)] and shares similar constellations of disease and health.
We should reckon on something similar with our data, just to check if it fits with the final goal of measuring health and wellbeing. As you may imagine, there are many implications. If we agree on a comprehensive model of health, then we have to focus on how decisions and priorities should be made.
The achievement of a human-made plan depends 1/4 on resources, such as money, education or physical strength; 1/4 on skill and decisions; and 1/2 on unpredictable circumstances, usually called luck. A student asked me how luck can be improved: well, I said, if you keep pursuing your goal with perseverance, the probabilities to get it increase (like if you keep playing the lottery, the probability to get the prize also increases)
Finally I've found a book that explains the concept of egalitarianism and its implications with a clear message.
Distributive justice is an area not only of philosophy, but also of several other academic disciplines. For example, the formal analysis of economics is extremely important and valuable for understanding the structure of egalitarian theories of distributive justice. However, it intimidates some people. I believe that the most fruitful way to present theories of distributive justice is to integrate the results of economics and political theory into philosophical analysis.
The concept:
Egalitarianism: a class of distributive principles, which claim that individuals should have equal quantities of well-being or morally relevant factors that affect their life.
What it is not egalitarianism, but maybe you are not aware of:
There are at least four well-known distributive principles that are not egalitarian in the sense I defined above, yet some people think that these are egalitarian in some sense.
The first example is utilitarianism. Utilitarianism can be defined in various ways. Take classical utilitarianism. Classical utilitarianism contends that an act is right if and only if it maximizes the total sum of people’s well-being in a given society. When we calculate the total sum, we assign equal weight to each person’s well-being and simply add up different people’s well-being. Classical utilitarianism endorses assigning equal weight
to every person’s well-being, and it might be claimed that it is egalitarian. However, it is not concerned with how people’s well-being is distributed. Thus, I do not consider it as a form of egalitarianism.
The second example is libertarianism.
The third is the Marxist principle of justice or communism
The fourth is the proportionality principle.
The book reviews several perspectives on egalitarianism with concrete descriptions and comments:
6 Equality and time
7 Equality in health and health care
The chapter on health is specially welcome and is a required reading for health economists, and for supporters of QALYs:
It is obvious that the principle of QALY maximization is utilitarian in spirit. It adds up different people’s good, and claims that we should choose the allocation that maximizes the total good. In the context of health care resource allocation, the good is QALY, which measures health benefit. QALY is added up across individuals to estimate the goodness of different outcomes. Then, the alternative that maximizes the goodness of outcome is chosen. It is not surprising that, according to QALY maximization, it does not matter how QALYs are distributed across individuals. Needless to say, all sorts of objections leveled against utilitarianism are raised against QALY maximization.
Usually, QALY maximization is understood as the unweighted sum of QALYs. However, it does not need to be so.We can make it a weighted sum and give priority to the worse off. If we give priority to the worse off, then it is possible to bring egalitarian concerns to bear on the allocation of health care resources.
One chapter is not enough to disentangle the complexities of QALYs, but it is worth reading.
At the end the author explains his position:
My preferred distributive principle is the aggregate view of telic egalitarianism. I am not
willing to support Rawls’s difference principle, because I agree with Harsanyi(1975) that the difference principle in practice ignores the benefits to the non worst off groups and therefore fails to secure the stability of the basic structure of society. This stands in opposition to Rawls’s claim that the difference principle, together with other principles of justice, guarantees a satisfactory minimum, and therefore secures the stability of the basic structure.
My view is coincidental with the author.
PS The concept of telic (telelological) egalitarianism:
There are two main ways in which we can believe in equality. We may believe that inequality is bad. On such a view, when we should aim for equality, that is because we shall thereby make the outcome better. We can then be called Teleological – or, for short, Telic – Egalitarians. Our view may instead be Deontological or, for short, Deontic. We may believe we should aim for equality, not to make the outcome better, but for some other moral reason. We may believe, for example, that people have rights to equal shares. (Parfit 2000: 84)
In deep endebted states, the endless debate about direct taxes finally relies on one thing, where is the money to raise more resources?. Nowadays, you'll notice a different formulation, focused on redistribution: we want to raise more money to redistribute to those with unfulfilled needs.
A new book is specially welcome to clarify all the concepts in a politicaly troubled moment:
We argue that societies do not tax the rich just because they are democracies where the poor outnumber the rich or because inequality is high. Nor are beliefs about how taxes influence economic performance ultimately decisive. Societies tax the rich when people believe that the state has privileged the wealthy, and so fair compensation demands that the rich be taxed more heavily than the rest.
When it comes to thinking of what tax policy is best, few would disagree with the notion that governments should be-in part guided by fairness. It is a term used frequently by those on both the political left and right.1 How can this be? History suggests that the concept of fairness is up for grabs. Standards of fairness in taxation vary greatly across countries, over time, and from individual to individual.
If we believe that
Political support for taxing the rich is strongest when doing so ensures that the state treats citizens as equals. Treating citizens as equals means treating them with "equal concern and respect".
Then, we'll agree that the current debate on taxing the rich in our country is absolutely biased and intentionally partisan. With this approach we can't build a new country.
What a country decides about taxes on the rich has profound consequences for its future economic growth and the distribution of economic resources and opportunities
Therefore, this is the book to read for those that have to prepare the next public budget, and for any citizen, a must read.
Most of us can remember the withdrawal of antiinflamatory drug Vioxx in 2004. And some of us still wonder about the FDA responsibility and its experts committees on that sad affair.
Criticism reached a peak in February 2005 following the work of a committee set up to determine whether or not two of Pfizer’s anti-inflammation medicines, CelebrexR and BextraR , should remain on the market and whether Merck’s anti-inflammation drug VioxxR could be approved again for marketing. The vote – a close one, slightly in favor of the highly controversial BextraR and VioxxR – surprised the informed public and raised suspicions, leading The New York Times to commission a study on committee members’ financial ties. It turned out that ten members (out of thirty-two) had financial ties with one or more drug companies, most with Pfizer (Harris and Berenson 2005; CSPI 2005). As the critics saw it, this was a sign that advisory committees themselves, like FDA’s top management before them, had come under the influence of the drug industry.
After that, the FDA changed its rules for voting to simultaneous and visual methods rather than oral. This option avoids the anchoring effect of first voters. But secret voting was never contemplated.
This is exactly the issue that is addressed in a chapter of the book Secrecy and Publicity in Votes and Debates and now that everybody backs transparency, it's a good moment to stop and read this chapter at least.
So although public voting may be preferred because it allows external actors to monitor expert behavior, secret voting may appear desirable as a means of preventing conformism among experts. Thus, the value of the voting method may depend on of the audience considered: other voters or external actors. There is, however, one procedure that reconciles the benefits of publicity and secrecy, and that is to vote secretly but reveal who voted how after the vote count has been recorded. This method, used in Dominican monasteries in the thirteenth century in a process called the scrutinium (Gaudemet 1979, p. 326) and recommended by Bentham (1999, p. 106), may be termed, following Jon Elster (2013), “secret-public voting.”
The FDA 2007 reform replaced public voting with secret-public voting, but it also replaced oral voting, which left ample opportunity for individual members to express
themselves, with “manual” followed by digital voting, which precludes all such expression.
These statements prompt many questions about how our close advisory committees are taking decisions. I don' know any detail about it. And details are important, specially if there are lives at stake.
A long long time ago Michael Porter wrote Competitive Strategy a book that has been used as the bible of strategy.
Porter’s model identifies five forces that affect the strategic position of a particular business: the threat of new entrants to the market, the threat of substitute products or services, the bargaining power of customers, the bargaining power of suppliers, and the intensity of competitive rivalry in the industry. The goal of strategy is to control these five forces in such a way as to build a moat around the business and thereby render it unassailable.
Thus, when a firm can erect barriers to entry, it can keep competitors out, and entrants with substitute products cannot storm the castle. When a firm can subjugate suppliers, competition among them weakens their bargaining power so the firm can keep its costs low. When a firm can subjugate buyers by keeping them relatively small, disunited, and powerless, the firm can keep its prices high.
In this model, the firm maximizes profits by avoiding ruinous competition for itself but encouraging it for everyone else in the value chain. Advantage is found in industry structures that create a protective moat—one that enables the firm to segment markets, differentiate products, control resources, avoid price wars, and defend its profit margins.
For decades, companies have studied the five forces model and used it to guide their decisions about which markets to enter and exit, what mergers or acquisitions to consider, what sorts of product innovation to pursue, and what supply chain strategies to employ.
Enter platforms. Many of the insights embodied in the five forces, resource-based, and hypercompetition models remain valid, but two new realities are now shaking up the world of strategy.
First, firms that understand how platforms work can now intentionally manipulate network effects to remake markets, not just respond to them. The implicit assumption in traditional business strategy that competition is a zero-sum game is far less applicable in the world of platforms. Rather than re-dividing a pie of more-or-less static size, platform businesses often grow the pie (as, for example, Amazon has done by innovating new models, such as self-publishing and publishing on demand, within the traditional book industry) or create an alternative pie that taps new markets and sources of supply (as Airbnb and Uber have done alongside the traditional hotel and taxi industries). Actively managing network effects changes the shape of markets rather than taking them as fixed.
Second, platforms turn businesses inside out, moving managerial influence from inside to outside the firm’s boundaries. Thus, a firm no longer needs to seize every new opportunity on its own; instead, it can pursue only the best opportunities while helping ecosystem partners seize the others, with all partners sharing the value they jointly create.13
These two new realities add a dramatic layer of complexity to business competition. Platform strategy resembles traditional strategy much the way three-dimensional chess resembles the traditional game.14 Within the ecosystem, the lead firm negotiates dynamic tradeoffs involving competition at three levels: platform against platform, platform against partner, and partner against partner.
These are excerpts from the book "Platform revolution" a must read if you want to understand what's going on in value creation in a connected world. In chapter 12 you'll find some comments on health sector, very succint and general.





















{kind=link}