According to the Gospels, a large crowd had gathered and was following Jesus. Jesus called his disciples to him and said:
"I have compassion for these people; they have already been with me
three days and have nothing to eat. I do not want to send them away
hungry, or they may collapse on the way."
His disciples answered:
"Where could we get enough bread in this remote place to feed such a crowd?"
"How many loaves do you have?" Jesus asked.
"Seven," they replied, "and a few small fish."
"Jesus told the crowd to sit down on the ground. Then he took the seven
loaves and the fish, and when he had given thanks, he broke them and
gave them to the disciples, and they in turn to the people. They all ate
and were satisfied. Afterward the disciples picked up seven basketfuls
of broken pieces that were left over. The number of those who ate was
four thousand men, besides women and children. After Jesus had sent the
crowd away, he got into the boat and went to the vicinity of Magadan (or
Magdala)."
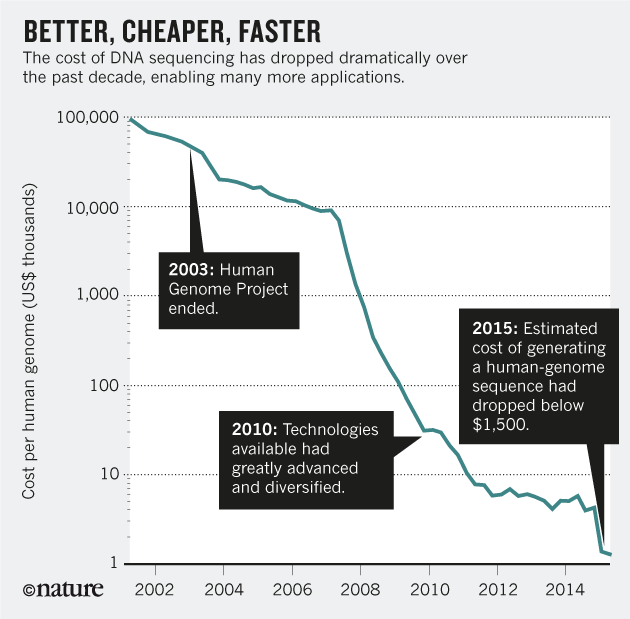
Now let's imagine one country and his health expenditure in 2007 and 2017, let's think about a figure, let's say 1,186€. This was the per capita expenditure in 2017. What was the per capita expenditure one decade earlier? 1€ less!!! It was 1,185€. This is a miracle, if you take inflation into account the reduction of expenditure is huge. Technology and ageing were not the drivers of expenditure growth because there was no growth!
Between 2017 and 2016 the growth was 5.9% in public expenditure. In private health insurance expenditure it was 5,4%. That's it.
If you have to think about health expenditure miracles, have a look at Catalonia, it's incredible.
And it is so incredible that today our government is in exile, or in prison, or bail pending trial. Today the spanish police has entered in our government palace and has arrested one high official.
This is the rogue state where the majority wants to leave, and unfortunately we are alone, prosecuted and it's not possible to decide the new president. Europe forgets the attack on civil liberties. Shame.
Now