If you want to know if some device is effective, there is a standard way to demonstrate it: a clinical trial. This is precisely what has been done on the impact of wearables on weight loss. And the result is:
Among young adults with a BMI between 25 and less than 40, the
addition of a wearable technology device to a standard behavioral
intervention resulted in less weight loss over 24 months. Devices that
monitor and provide feedback on physical activity may not offer an
advantage over standard behavioral weight loss approaches.
That's amazing! Why is there so many articles pushing wearables for weigth loss when there are very few clinical trials, and their results are clearly against their use?. This is a marketing bubble and somebody should tell clearly that they could use wearables but for other reasons.
PS. Let's imagine that somebody wants to relate wearables for weight loss reduction with insurance premiums! Nothing to add.
If there is an example of how one part of an organization can't speak with the other is the European Union and Health Policy. If we are talking about medical devices, health issues are at the back, industry is writing the regulations. If we are talking about options for improvement, economics unit explains what health unit has to do. A perfectly designed mess.
Take the example of this week. A Joint report, that is an economics report with elementary mistakes for any health economist. Take this statement:
"Competition between hospital providers can lead to higher quality under strict price regulation." (p.70)
Does anybody know what does really mean strict regulation? Who is writing such things and being paid with our taxes?.
If you check another report on the topic by experts of the European Union you'll find an opposite recomendation.
"The conditions for competition to be a useful instrument vary across countries, health care subsectors and time. There is no golden rule or unique set of conditions that can be met to ensure that competition will always improve the attainment of health system goals." (p.4)
Definitely, the EU is in the middle of no judicious health policy.
In summary, an avoidable report that you can skip reading and devote your time to hearing Bob Dylan music for example, the new Nobel Prize.
Come gather 'round people where ever you roam
And admit that the waters around you have grown
And accept it that soon you'll be drenched to the bone
If your time to you is worth savin'
Then you better start swimmin' or you'll sink like a stone,
For the times they are a' changin'!
Come writers and critics who prophesy with your pen
And keep your eyes wide the chance won't come again
And don't speak too soon for the wheel's still in spin
And there's no tellin' who that it's namin'
For the loser now will be later to win
For the times they are a' changin'!
Come senators, congressmen please heed the call
Don't stand in the doorway don't block up the hall
For he that gets hurt will be he who has stalled
There's a battle outside and it's ragin'
It'll soon shake your windows and rattle your walls
For the times they are a' changin'!
Come mothers and fathers throughout the land
And don't criticize what you can't understand
Your sons and your daughters are beyond your command
Your old road is rapidly agin'
Please get out of the new one if you can't lend your hand
For the times they are a' changin'!
The line it is drawn the curse it is cast
The slow one now will later be fast
As the present now will later be past
The order is rapidly fadin'
And the first one now will later be last
For the times they are a' changin'!
After all these years, a new proposal for regulating in vitro diagnostics and medical devices in EU is available. Current regulation was enacted in 1998, and this one could be applicable in 2022, 24 years after, pas mal for the busy politicians!.
And this is a proposal, there were previous unapproved proposals, and this one has to pass the Council and the Parliament. I will not enter into the details.
It was supposed to increase safety and efficacy, but the main problem remains with who has to enforce them. Notified bodies, a subcontracting regulatory firms network, with vested interests with industry can't claim independence. And specifically, the methods for evaluate the analytical validity, clinical validity and utility is uncertain. No regulator will confirm us that the cut-off values of diagnostic tests are set according to the best evidence and greatest benefit. In US, FDA is the responsible.
In summary, a new missed opportunity for european citizens. A greater risk and uncertain effectiveness in diagnostic tests and medical devices.
PS. The latest known example of the impact of wrong regulation is this one. Those affected can't read this blog, they are blind.
Cost-effectiveness may be considered a focal point for health economists. However the trip from theory to implementation raises many doubts. The reductionist perspectives of some health economists consider that politicians are rational in decision making. And this is not the case. I suggest you a look at this article:
The cost-effectiveness model generally used for the evaluation of health technologies—and health care and public health interventions more widely—has become a central tool for public-sector policy makers in many health care systems. It was developed to help decision makers with fixed public resources to compare (1) different interventions for the same health problem and (2) programs in different disease areas. For a particular level of health care resources, the goal is to
choose from among all possible combination of programs the set that maximizes total health benefits produced. The traditional CEA methods presume the existence of only one salient constraint— the public finance budget constraint. Yet all of the evidence suggests that many other constraints impinge on decision makers, at least in the short run.
A fundamental reason for the failure to implement is that CEA assumes a single constraint, in the form of the budget constraint, whereas in reality decision makers may be faced with numerous other constraints. The objective of this article is to develop a typology of constraints that may act as barriers to implementation of cost-effectiveness recommendations. Six categories of constraints are considered: the design of the health system; costs of implementing change; system interactions between interventions; uncertainty in estimates of costs and benefits; weak governance; and political constraints.
There is intelligent life beyond cost-effectiveness...
All what you need to know about the implications of stratified medicine, you can get it in one article. That's great. And at the same time worrying or amazing for somebody. You'll see that stratified medicine reduces the size of the market with the use of biomarkers. Than, more accuracy is more costly. However, who sets the cut-off? This is the question. Trusheim and Berndt shed light on the issue:
Setting the cut-off value for the imperfectly performing companion diagnostic presents multiple challenges to the scientist, regulator, ethicist, marketer, clinician, and payer. Scientists might seek natural break points connected to a biological mechanistic rationale, or struggle to define the proper balance between diagnostic sensitivity and specificity. Regulators might seek a division that maximizes the benefit:risk ratio with the greatest certainty. Ethicists might be concerned with issues of denying care to some or knowingly causing harm to some (statistically) to benefit others. Marketers might seek to optimize revenues by balancing efficacy improvements, and the correlated pricing and market share, with the number of eligible patients in the market. Clinicians might seek to know the likelihood that their individual patient will respond to treatment or will incur an adverse event. Payers might focus on the net clinical benefit to their specifically covered population and the overall affordability of the resulting net total outlays for the actually treated population. Although clearly having overlapping perspectives, when selecting the CDx cut-off each stakeholder brings its own unique view of the issues to emphasize and the proper metrics to optimize.
Meanwhile, you'll not be able to find any implication of the regulator on selecting the right cut-off in the new european draft rules for in vitro diagnostic tests. This is a new missed chance.
Today I'll suggest a reading from the latest issue of Nota d'Economia. You'll find two articles of special interest for health economists. The first one, on institutional design will convince you that this is the tough part of the issue. Governments prefer to avoid difficult decisions, only a proper institucional design will provide the best impact of economic evaluation. The second one is an excellent example of the impact of stroke prevention and care, or how organizational innovation may deliver social value of 372M€ in 7 years. Great, we need more initiatives like that, and studies that assess its impact.
This is the summary:
Aquest estudi mostra que després de les millores que han tingut lloc en l’atenció a l’ictus agut a Catalunya (Abilleira et al., 2009, 2011a, 2011b; Salvat-Plana et al., 2011) en el període 2005-2012 es van evitar 719 defuncions i es van guanyar 11.153 anys de vida, amb un valor social mínim de 353.164.622,08 euros (1.050.147.483,07 euros màxim). Un cop eliminat l’efecte de l’augment de la incidència, el nombre de defuncions per ictus va ser de 919 i 11.760 anys de vida guanyats, amb un valor social mínim de 372.404.624,76 euros (1.195.167.115,79 màxim)
PS. US is affraid of economic evaluation...have a look at JAMA
What happens if "one quarter of the clinical genetic results from commercially available multiplex cancer panels and reported at the PROMPT registry had conflicting interpretations" and if "36% of conflicting genetic tests results appeared to be clinically relevant, because they were either reported as pathogenic/likely pathogenic"? Does anybody care about it?.
I would suggest today you have a look at this article and your level of anxiety will increase suddenly.
Clinical data and genetic testing results were gathered from1,191 individuals tested for inherited cancer susceptibility and self-enrolled in PROMPT between September 2014 and October 2015. Overall,participants (603 genetic variants) had a result interpreted by more than one laboratory, including at least one submitted to ClinVar, and these were used as the final cohort for the current analysis.
Of the 603 variants, 221 (37%) were classified as a variant of uncertain significance (VUS), 191 (32%) as pathogenic, and 34 (6%) as benign. The interpretation differed among reporting laboratories for 155 (26%). Conflicting interpretations were most frequently reported for CHEK2 and ATM, followed by RAD51C, PALB2, BARD1, NBN, and BRIP1. Among all participants, 56 of 518 (11%) had a variant with conflicting interpretations ranging from pathogenic/likely pathogenic to VUS, a discrepancy that may alter medical management.
Therefore,
Clinical interpretation of genetic testing for increased cancer susceptibility as assessed by multiplex panels hinges on accurate curation and interpretation of variants. Discrepant interpretation of some genetic variants appears to be common.
Take care. The regulator remains on vacation, a never ending vacation.
Diagnostic tests show
different levels of false positive and negatives in the results. The
impact of such unwanted results by physicians finally have an impact on
health and quality of life of patients. You can check what does this
means for HER-2 test in breast cancer in US in this article.
Patients
with breast cancer whose tumors test positive for human epidermal
growth factor receptor 2 (HER2) are treated with HER2-targeted therapies
such as trastuzumab, but limitations with HER2 testing may lead to
false-positive (FP) or false-negative (FN) results.
Among 226,870
women diagnosed with EBC in 2012, 3.12% (n = 7,070) and 2.18% (n =
4,955) were estimated to have had FP and FN test results, respectively.
Approximately 8400 QALYs (discounted, lifetime) were lost among women
not receiving trastuzumab because of FN results. The estimated
incremental per-patient lifetime burden of FP or FN results was $58,900
and $116,000, respectively. The implied incremental losses to society
were $417 million and $575 million, respectively.
Absolute
certainty in diagnosis is unattainable, no matter how much information
we gather, how many observations we make, or how many tests we perform. A
diagnosis is a hypothesis about the nature of a patient's illness, one
that is derived from observations by the use of inference. Our task is
not to attain certainty, but rather to reduce the level of diagnostic
uncertainty enough to make optimal therapeutic decisions.
USA is well known for its prominent interest in avoiding cost-effectiveness as we know in certain european countries. They talk about comparative effectiveness research, because it fits with their current priorities: What works best? and let's the cost for another day. Forget trade-offs.
If you want to know the recent stuff on the topic, have a look at this article. You'll notice three steps: clinical care value, managing affordability and health system value. It makes sense as a first step. In our country we don't have such official estimates. The next step should be to introduce cost and equity considerations.
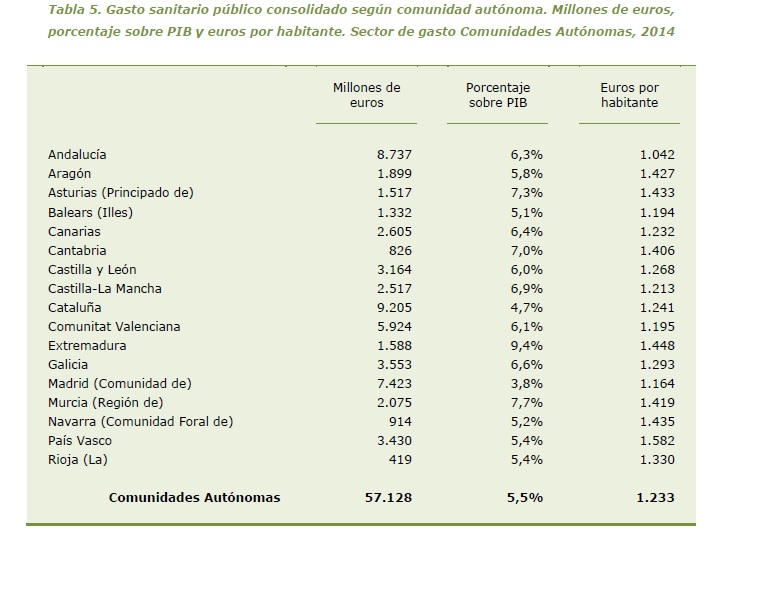
Let's imagine an alleged State. All its citizens pay taxes under the same Tax Code. Health Benefits are the same under the Health Act. And spending on health care according to geography, can reach 52% more in Basque country compared to Andalusia. This is not new. Many decades having the same figure and nobody cares about it.
This is an easy table to understand health policy making in a failed state. Catalonia spends 4,7% of GDP on health, other sources say 5,5%. Anyway, you'll not find an OECD country with similar figures. After a decade we are spending the same amount per citizen than in 2006, 1.120 €. I will not add anything to this mess. There is only an increasing need to disconnect. Is there any MP in the room?
PS. I'm not arguing that every country has to spend the same, I'm just saying that it is not legally possible to deliver the same benefits with such different budgets. Therefore we are unequal before law. This is the usual legal uncertainty of a failed state.
JAMA has decided to start JAMA Professionalism, a new department.
The goal of the articles in this section is to help physicians fulfill required competencies on this topic. According to the American Board of Medical Specialties definition, professionalism is “…a commitment to carrying out professional responsibilities, adherence to ethical principles and sensitivity to diverse patient populations.” Taking responsibility for executing professional responsibility seems intuitive enough. But what does it mean to adhere to ethical principles? How are the ethical principles defined?
Good questions. And the answers for US physicians are in the new AMA Code of Medical Ethics.
A multi-year effort to modernise that has provided an interesting outcome. You can check for example, regarding prioritisation of resources, what should be done? in chapter 11 you'll find the answers. A good suggestion for our physicians' associations and their outdated codes.
How do you want to manage, with a rearview mirror or just looking forward? Big data allows to look forward with better precision. The uncertainty about the disease and about the cost of care is large when you enter in hospital from an emergency department. But, after the diagnosis (morbidity), could we estimate how much could cost an episode?. If so, then we could compare the expected cost and the observed cost on a continous process.
Right now this is possible. Check this article that we have just published and you'll understand that costs of different services according to morbidity can be reckoned and introduced in health management. This analysis goes beyong our former article, much more general. So, what are we waiting for? Big data is knocking at the door of health care management, predictive modeling is the tool.
Amazing concert by Caravan Palace in Sant Feliu de Guixols three weeks ago.