Sustainability defined by OECD (p.25):
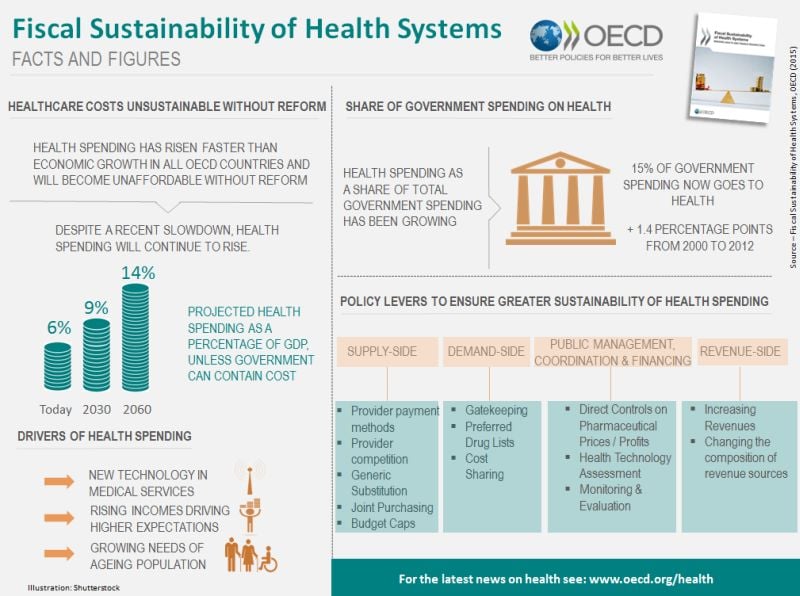
The OECD defines fiscal sustainability as the ability of a government to maintain public finances at a credible and serviceable position over the long term (OECD, 2013). Fiscal sustainability implies governments are able to maintain policies and expenditure into the future, without major adjustments and excessive debt burdens for future generations. The term refers to overall government spending, revenues, assets and liabilities that reflect past commitments and adapt to future trends such as socio-economic trends and environmental factors.
For the health sector, fiscal sustainability is perhaps best understood as a constraint that needs to be respected, rather than an objective in itself (Thomson et al., 2009). This implies that how governments achieve fiscal sustainability matters, rather than it becoming a simple cost-cutting exercise.Of course!. Sometimes OECD writes obvious statements. There is a budget constraint! Perhaps someone has forgotten it.
I understand that in some countries the budget is not credible, because its health basket is more generous and prices are higher compared to the available resources. Is this a reason to complain about cutbacks?. If there is a budget, the role of any politician is to comply with the budgetary constraint, they must prioritise. Health care is not an excuse to surpass the budget and responsible citizens and parties should acknowledge it.