The times for drug prescription following prioritisation have arrived. Hepatitis C drugs have paved the way for such a move.There were some informal attempts for certain medicines and it was decided by clinical committees (i.e. for rare diseases), but now it has changed. The government has decided who has to get what and when, this is absolutely new. Have a look at this draft of strategic therapy for Hepatitis C treatment.
Any physician asking for hepatitis C drugs will have to explain the compliance with the criteria and ask for approval.
I said some weeks ago that a new paradigm in drug pricing was starting, right now I have to say that drug prescription priorisation by rules is the new trending topic, at least in our neighbourghood. Wether this prioritisation is based by cost-effectiveness criteria remains to be seen.
Es mostren les entrades ordenades per rellevància per a la consulta hepatitis. Ordena per data Mostra totes les entrades
Es mostren les entrades ordenades per rellevància per a la consulta hepatitis. Ordena per data Mostra totes les entrades
07 de novembre 2014
16 d’abril 2025
Pooling plasma, quin desastre! (2)
El llibre "Blood on Their Hands: How Greedy Companies, Inept Bureaucracy, and Bad Science Killed Thousands of Hemophiliacs" d'Eric Weinberg i Donna Shaw, publicat el 2017, documenta la tragèdia de com milers de persones amb hemofília van resultar infectades amb el VIH a causa de productes sanguinis contaminats, assenyalant com a principals responsables a empreses avaricioses, una burocràcia incompetent i una ciència deficient.
El llibre es basa en la investigació d'Eric Weinberg, un advocat que va representar a moltes de les víctimes i les seves famílies. La prefaci comença amb el funeral de Joe Salgado, un amic de Weinberg que va morir a causa de la infecció per VIH adquirida per tractaments per a l'hemofília, establint la connexió personal de l'autor amb la comunitat afectada.
La taula de continguts revela l'estructura narrativa del llibre, que abasta des dels orígens de la producció de productes sanguinis fins a les conseqüències legals i personals de l'epidèmia.
- La secció "Beginnings" (Capítol 2) probablement explora la història primerenca del tractament de l'hemofília i el desenvolupament dels concentrats de factor.
- "How Could It Happen and Nobody Did Anything Wrong?" (Capítol 3) planteja la qüestió central de la responsabilitat.
- "A History Ignored" (Capítol 4) examina el context històric, possiblement detallant advertències i riscos que es van ignorar. Es menciona que es va identificar un sistema de donació de sang totalment voluntari com una de les millors maneres de reduir el risc, però va trobar resistència per part de gairebé tothom. També es discuteix com la comunitat d'hemofílics va començar a veure les implicacions de donar la iniciativa a la indústria en lloc dels bancs de sang i hospitals. Robert Massie, autor d'un llibre sobre la criança d'un fill amb hemofília, inicialment tenia grans esperances que la Creu Roja Americana produís concentrats de Factor VIII, però això no va passar.
- "Digging In" (Capítol 5) descriu la investigació de Weinberg, que va incloure la descoberta de documents importants, com ara un informe de 1976 titulat "Unsolved Therapeutic Problems in Hemophilia" que va organitzar el Dr. Aronson, considerat crític per al cas. Aquest informe abordava un virus desconegut anomenat hepatitis no-A, no-B, que es transmetia als pacients amb hemofília. Weinberg també va decidir anar a Alemanya per obtenir més informació sobre Behringwerke.
- "Reaching Out" (Capítol 6) narra els esforços de Weinberg per connectar amb altres advocats i possibles aliats en la lluita legal, com David Shrager.
- "Help Wanted" (Capítol 7) tracta sobre la cerca d'ajuda i recursos per al cas, incloses les interaccions amb l'Associació d'Hemofília de Nova Jersey (HANJ) i la seva directora executiva, Elena Bostick. HANJ va acceptar una oferta de patrocini d'un seminari amb la condició que s'hi convidés a tots els advocats involucrats en litigis d'hemofília a Nova Jersey, que en aquell moment era només Weinberg.
- "All for Business" (Capítol 8) explora com els interessos comercials van influir en les decisions relacionades amb la seguretat dels productes sanguinis. Weinberg va contactar amb el Dr. Shanbrom, que tenia patents relacionades amb l'hemofília, per investigar si hi havia tecnologia disponible per netejar els productes de factor abans que el VIH contaminés el subministrament de sang.
- "Somewhere Here, I Have the Documents" (Capítol 9) se centra en la dificultat d'obtenir proves i documents clau.
- "More Lawyers, More Experts" (Capítol 10) detalla la construcció de l'equip legal i la cerca de testimonis experts. Weinberg es va reunir amb el Dr. Dubin per revisar informació sobre els seus clients. També va haver de buscar en la literatura mèdica referències a la necessitat de netejar els fàrmacs de coagulació. Va trobar un article clau al New England Journal of Medicine de 1978 que alertava sobre malalties hepàtiques en hemofílics i instava la indústria a netejar els concentrats. El Dr. Van Thiel, un dels autors, va acceptar ser un testimoni expert.
- "A Meeting with Roger" (Capítol 11) descriu trobades i estratègies legals.
- "An Act of Man" (Capítol 12) probablement examina les accions i omissions individuals que van contribuir a la tragèdia.
- "The Trouble with Torts" (Capítol 13) aborda les complexitats del dret de danys en aquest tipus de litigis.
- "I Murdered My Child, But Not Alone" (Capítol 14) ofereix una perspectiva personal i devastadora de les conseqüències de la contaminació.
- "Of Sheep and Men" (Capítol 15) i "A Failure of Leadership" (Capítol 16) analitzen la responsabilitat de la indústria i les autoritats reguladores. Es menciona que Baxter utilitzava plasma recollit de presons, incloent-hi la Penitenciaria Estatal de Louisiana a Angola. També es detalla com els executius d'Armour van decidir no notificar a la FDA sobre les dades del Dr. Prince i van continuar venent Factorate. El govern federal estava preocupat pel risc d'hepatitis d'un producte de coagulació sanguínia de Hyland ja el 1968, però la companyia no entenia la preocupació. Behringwerke AG a Alemanya estava provant un producte de coagulació tractat amb calor el 1979, cosa que va fer que Baxter tornés a posar la investigació sobre l'hepatitis a la seva llista de prioritats "A".
- "From Prime Chuck to Dogeza" (Capítol 17) i "Endings" (Capítol 18) narren les conclusions dels processos judicials i les seves resolucions. Es menciona l'aprovació de la llei Ricky Ray Hemophilia Relief Fund Act per la Cambra de Representants dels EUA.
- L'epíleg ofereix reflexions finals sobre la tragèdia i les seves implicacions per a la seguretat del subministrament de sang en l'actualitat.
En resum, "Blood on Their Hands" és un relat detallat de la crisi de la contaminació per VIH dels productes de factor VIII utilitzats per tractar l'hemofília als Estats Units. El llibre exposa com els guanys empresarials van prevaldre sobre la seguretat del pacient, com la ineptitud burocràtica no va poder prevenir la propagació de la infecció i com la mala ciència i la manca de diligència van contribuir a la mort de milers de persones. A través de la investigació de Weinberg i les històries personals de les víctimes, el llibre ofereix una acusació contundent de les falles sistèmiques que van conduir a aquesta tragèdia.

24 de febrer 2023
La teranyina que sosté la financialització dels medicaments, la salut i la vida
Capitalizing a Cure. How Finance Controls the Price and Value of Medicines
Acabo de llegir un llibre d'accés obert com fa temps que no en trobava cap d'igual. Es tracta d'un treball molt detallat de com el sofosbuvir va sorgir i es va introduir al mercat per capgirar l'Hepatitis C. És un esforç que en Victor Roy, metge i sociòleg, ha estat fent durant molts anys amb un resultat impecable. Va de la financialització dels medicaments, la salut i la vida. Esdevé una peça clau per entendre el que està passant amb el preu dels medicaments i els seus motius. Ho explica amb tot detall i bàsicament el missatge és: si no fem res, això anirà a més. És a dir a preus estratofèrics que uns diuen que es relacionen amb el valor (els mateixos que posen el preu) i uns altres que arribats a un cert punt ja no podem entendre res.
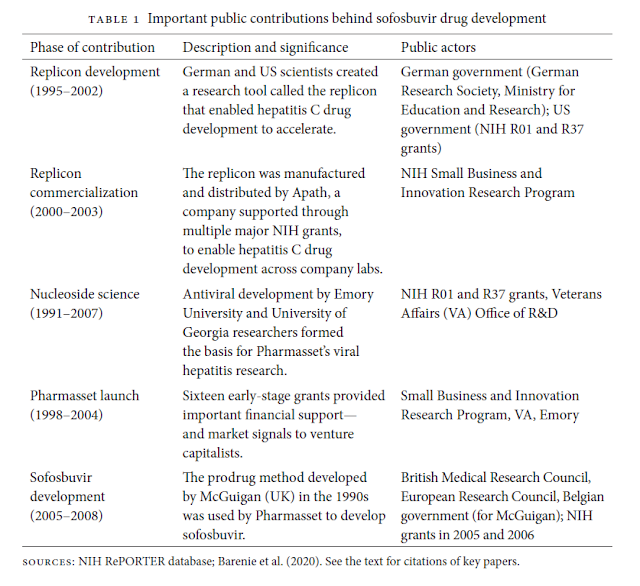
Sobre la qüestió de que els preus són alts per recuperar la inversió en R+D, cal explicar dues coses. En el cas del sofosbuvir la contribució a la recerca finançada públicament va ser determinant. Aquí hi ha un resum:
I la segona. Sobre si l'empresa comercialitzadora va fer Recerca o Cerca, en realitat es va dedicar a cercar mol·lècules com actius financers i va deixar de banda el risc de la recerca en estadis inicials. Per tant es va substituir la R+D per la C+D.
El resum és una empresa, Pharmasset, que el seu funcionament va costar 314 milions entre 1999 i 2011:

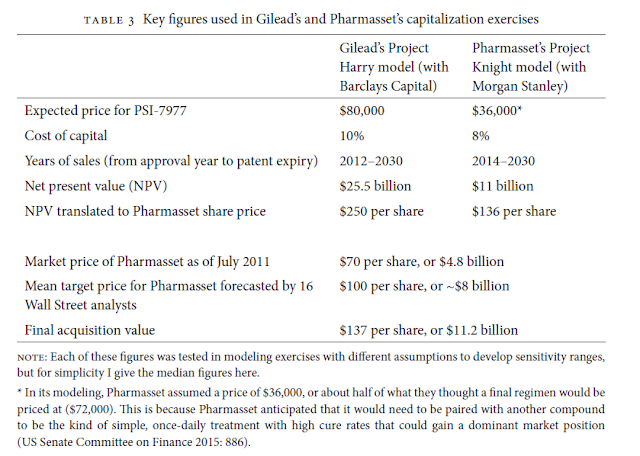
I que havia dedicat només 62 milions a la recerca en el sofosbuvir. El 2010 ja es valorava en 5.000 milions sense tenir cap producte al mercat, ni facturació. El 2011 Pharmasset seria comprada per 11.200 milions.
El resum dels dos escenaris al moment de la compra és aquest:
I a la pregunta, què va costar la recerca del sofosbuvir? El quadre següent ho diu tot:

Va costar menys de 1.000 milions en finançament privat, el finançament públic és complex detallar-lo encara que el llibre explica les fonts, que eren nordamericanes i europees.
El sofosbuvir va suposar un canvi en molts aspectes, tant clínics com econòmics. El llibre ho explica amb molta precisió. Parla de creació de valor, però sobretot d'extracció de valor i com es produeix.
Sobre el mecanisme de preus i com es genera l'escalada de preus dels medicaments, aquest gràfic ho mostra clarament:

L'argument del llibre és que els preus que observem són fruit d'un disseny financer que estableix expectatives de preu i creixement futur, això és Wall Street i NASDAQ. El segon element que afegeix incentius desmesurats és el sistema de patents i el monopoli que atorga. Per tant la indústria farmacèutica es troba dins aquesta teranyina i la pregunta clau és com sortir-ne de tot plegat.
La resposta de Victor Roy es troba als darrers capítols on reflexiona sobre el paper públic de la investigació, com finançar públicament la recerca i llicenciar privadament la fabricació. Una qüestió sobre la que s'ha debatut molt i s'ha fet molt poc.
La meva recomanació és que ho llegiu i rellegiu amb deteniment, us ajudarà a comprendre el món complex al que ens enfrontem i que si no hi fem res, el desgavell està assegurat. I quan dic desgavell em refereixo més enllà del col·lapse econòmic a la sanitat, a l'accés inequitatiu a serveis de salut essencials i necessaris. Els incentius estan alineats per tal que es compliquin encara més les coses en el futur.
PD. Aquest és un llibre basat en fets i dades. Aquells que espereu un llibre sectari, (contra les farmacèutiques) no cal que el llegiu. No trobareu cap referència a la paraula-concepte neoliberalisme. L'aportació que fa el bengalí Victor Roy és extraordinària precisament per això, perquè evita qualsevol prejudici ideològic, una qüestió que cansa molt als nostres dies, massa.
PS. Resum del llibre amb IA.
El llibre Capitalizing a Cure: How Finance Controls the Price and Value of Medicines (2023), de Victor Roy, investiga detalladament el poder de les finances sobre la biomedicina i la salut pública. Utilitza com a cas d’estudi paradigmàtic el llançament dels tractaments curatius per a l'hepatitis C (VHC) el 2013, els preus dels quals (el "xoc d'adhesius") van intensificar el debat global sobre l'accés a nous medicaments.
La tesi central de Roy és que la crisi d'accés i els preus sense precedents d'aquests medicaments es deuen a la penetració del capitalisme financeritzat en el desenvolupament de fàrmacs. Sota aquest sistema, els medicaments curatius es converteixen en actius financers dominats per estratègies d'especulació i extracció de valor, que es produeixen a expenses de l'accés i la cura dels pacients.
I. Mecanismes de la Financerització i l’Assetització
Roy traça el viatge dels tractaments de l'hepatitis C basats en el sofosbuvir a través de quatre etapes clau:
1. Capitalització de la Ciència: Conversió del Coneixement Públic en Actius (Capítol 1)
El desenvolupament de la ciència darrere del sofosbuvir va ser un procés acumulatiu i col·lectiu que va dependre en gran mesura de la inversió pública.
- Innovació Pública Clau: El desenvolupament de la investigació sobre el VHC va ser possible gràcies a les inversions dels EUA i Alemanya, incloent-hi la creació de l'eina de recerca coneguda com a "replicon". El replicon va permetre accelerar dràsticament les proves de compostos antivirals i va ser crucial per orientar la innovació cap a teràpies curatives.
- Assetització: La companyia Pharmasset va ser fundada explícitament per Ray Schinazi per crear "actius farmacèutics" que poguessin ser venuts a companyies més grans. Aquesta pràctica de convertir el coneixement col·lectivament desenvolupat en actius financers privats es va fer possible gràcies a la llei Bayh-Dole Act (1980), que va permetre a universitats (com Emory) patentar recerca finançada amb fons federals.
- Desenvolupament del Sofosbuvir: El compost clau, PSI-7977 (sofosbuvir), va ser desenvolupat per Michael Sofia a Pharmasset, aplicant el mètode "prodrog" (phosphoramidate). Aquesta estructura es va basar en coneixement públic i disponible, desenvolupat prèviament per científics com Christopher McGuigan (Regne Unit).
- Valoració Especulativa: Tot i que Pharmasset no tenia productes aprovats i acumulava 330 milions de dòlars en dèficit al 2011, la seva valoració de mercat va superar els 4.800 milions de dòlars [60tab., 126]. Aquesta valoració no reflectia els costos de R+D (només 62,4 milions de dòlars per a sofosbuvir), sinó la predicció de creixement alimentada per les altes expectatives de preus futurs (l'anomenada "escala de preus").
2. Capitalització dels Medicaments: Poder Accionarial i Extracció de Valor (Capítol 2)
Gilead Sciences va adquirir Pharmasset el 2011 per 11.200 milions de dòlars, gairebé el triple del seu preu de mercat anterior, en una aposta financera massiva per adquirir creixement (Project Harry) [13, 60tab., 63, 109, 153n50, 154n76].
- Lògica de "Search and Development": Aquesta adquisició reflectia la tendència de la indústria a abandonar la recerca i el desenvolupament (R+D) interna i, en canvi, a enfocar-se en l'adquisició d'actius prometedors d'alt creixement per satisfer els seus accionistes.
- Rendiment Financer Extrem: Els tractaments de sofosbuvir van generar més de 46.000 milions de dòlars en ingressos durant els primers tres anys de vendes.
- Extracció de Rendes (Rents): La major part d'aquest benefici es va destinar als accionistes. Entre 2014 i 2016, Gilead va gastar més de 32.000 milions de dòlars en pagaments (dividends i recompra d'accions). Aquesta extracció es basa en la noció de renda (ingressos no guanyats) derivada del monopoli de la propietat intel·lectual i la ideologia de maximitzar el valor per a l'accionista.
3. Capitalització de la Salut: El Debat del Valor i la Crisi d’Accés (Capítol 3)
El llibre exposa, amb detalls dels documents interns de Gilead revelats per una investigació del Senat dels EUA, com la companyia va establir i justificar el preu dels medicaments.
- Fixació del Preu: El preu de llançament per a la teràpia combinada de sofosbuvir als EUA va ser de 94.500 dòlars per un tractament de tres mesos (el "píndola de 1.000 dòlars al dia").
- Càlcul: El preu es va basar en un "pis de preus" (preus dels tractaments anteriors, que ja superaven els 83.000 dòlars) i un "valor premium" justificat per la millor eficàcia, tolerabilitat i curta durada [76, 77fig., 180, 182, 184].
- Hegemonia del Valor: Gilead va impulsar una narrativa que afirmava que el preu reflectia el "valor econòmic de la salut futura" (estalvis en trasplantaments de fetge i hospitalitzacions). Aquesta justificació va ser reforçada per l'ús de la "ciència de la valoració" (estudis de cost-efectivitat basats en Quality-Adjusted Life Years o QALYs) per legitimar els preus en cercles acadèmics i polítics.
- Racionament de l'Atenció: El preu va provocar una crisi d'accés, amb sistemes de salut (com Medicaid i el sistema penitenciari dels EUA) racionant el tractament només als pacients en les etapes més avançades de la malaltia. Analistes de Wall Street van arribar a suggerir que el racionament podria ser "millor a llarg termini" per als ingressos de Gilead, ja que mantindria el mercat de pacients viu durant més temps.
- Poder de Contrarestació (Countervailing Power): L'accés divergent va dependre de la capacitat dels actors públics i de la societat civil per contrarestar el monopoli de Gilead. Mentre que als països d'ingressos alts es va racionar, països com Egipte van aconseguir negociar preus de 900 dòlars per tractament i van llançar campanyes massives. Gilead va oferir llicències voluntàries (que permetien produir genèrics a 1.000 dòlars) només a països de baixos ingressos, excloent inicialment milions de pacients en països d'ingressos mitjans.
- El Penyal del Pacient (Patient Cliff): L'èxit curatiu dels fàrmacs (taxa de curació del 90%) va conduir a una paradoxa en el model financeritzat: va reduir el nombre de pacients que necessitaven tractament, provocant una desacceleració del creixement i una caiguda de la cotització de Gilead. Per compensar, Gilead va intensificar l'extracció de valor i es va centrar en la seva lucrativa i crònica franquícia de VIH (medicaments de tractament de per vida).
IV. La Crisi i la Visió de Salut amb Propòsit Públic (Capítol 4 i Conclusió)
El llibre conclou que la financerització de la biomedicina produeix una "triple crisi": d'accés, per a futurs avenços (especialment cures), i per a la governança pública.
- Penalització de la Cura: El model actual incentiva els tractaments crònics (mitigators) que generen ingressos recurrents i sostenibles per sobre de les cures d'una sola presa. Aquesta és la raó per la qual Wall Street veu el creixement d'una empresa com Gilead com un "perill".
- Preus Desconnectats de la R+D: Les dades mostren que els preus dels fàrmacs no es basen en els costos d'R+D, sinó que estan lligats a les expectatives de beneficis dels mercats financers.
- Sistema de Propòsit Públic: Roy advoca per un canvi cap a un sistema de R+D amb propòsit públic, que intencionadament prioritzi l'accés assequible i la inversió en medicines que abordin les necessitats no satisfetes de salut. Aquest model requeriria:
- Inversions públiques completes (Opció Pública): L'Estat hauria de finançar totes les etapes del desenvolupament, assegurant que els medicaments es venguin a un preu proper al cost de fabricació.
- Govern del Valor: L'Estat ha d'utilitzar el seu poder com a principal comprador (countervailing power) per negociar preus assequibles i aplicar polítiques de patents socialment responsables.
- Ciència Oberta (Open Science): Promoure la col·laboració i l'intercanvi de dades per accelerar la innovació i reduir la redundància, en lloc de l'ús de patents per controlar el coneixement com un actiu.
El llibre conclou que la revaloració de la salut exigeix passar de capitalitzar la vulnerabilitat a valorar l'atenció equitativa i assequible per a tothom.

24 d’abril 2015
A successful implementation of a bad idea
Since 2012 it hasn't been posible to know the price of new drugs funded by NHS. The government considers that they are confidential. This is a clear example of what exactly means transparency and the application of the rule of law. Meanwhile a new strategy has been put into place. Without public prices, the government has decided to set budget ceilings for several innovative drugs: pertuzumab, ivakaftor, telaprevir/simeprevir, abiraterona, pirfenidona y ruxolitinib. And the last one is new drugs for hepatitis C, defined as "therapeutic group" not as a specific molecule. Following this strategy there is a proposal to extend such a model of budget ceilings by ATC, therapeutic classification.
This is really a bad idea that is already being implemented. As you know sometimes there are good ideas badly implemented, and therefore criticized. But in this case, it is a bad idea with a scrupulous implementation. Some officials consider that if they set a budget ceiling, all decisions will be taken to fit in with it. Clinical decisions follow a different path, not the mechanical and administrative way officials are used to.
The measure represents a tough hit to economic evaluation, because in the next future the government will not be any longer interested in it. Why? Their only concern is about the budget ceiling, the value doesn't matter. A missed opportunity for the development of priority setting under a rational scheme. Health economists should react to such a big mistake.
The saddest issue is that nobody knows what will happen when the budget ceiling is surpassed. This will be the job for the next government, nobody cares about it right now. Democracy and rule of law are only words subject to interpretation.
PS. All the details about hepatitis C controversy at Boletín AES.
PS. Understanding the foundations of confidential drug pricing, in Forbes.
PS. Explained at Health Affairs:
A
This is really a bad idea that is already being implemented. As you know sometimes there are good ideas badly implemented, and therefore criticized. But in this case, it is a bad idea with a scrupulous implementation. Some officials consider that if they set a budget ceiling, all decisions will be taken to fit in with it. Clinical decisions follow a different path, not the mechanical and administrative way officials are used to.
The measure represents a tough hit to economic evaluation, because in the next future the government will not be any longer interested in it. Why? Their only concern is about the budget ceiling, the value doesn't matter. A missed opportunity for the development of priority setting under a rational scheme. Health economists should react to such a big mistake.
The saddest issue is that nobody knows what will happen when the budget ceiling is surpassed. This will be the job for the next government, nobody cares about it right now. Democracy and rule of law are only words subject to interpretation.
PS. All the details about hepatitis C controversy at Boletín AES.
PS. Understanding the foundations of confidential drug pricing, in Forbes.
PS. Explained at Health Affairs:
International Best Practices For Negotiating 'Reimbursement Contracts' With Price Rebates From Pharmaceutical Companies
By: Morgan, Steven; Daw, Jamie; Thomson, Paige
HEALTH AFFAIRS Volume: 32 Issue: 4 Pages: 771-777 Published: APR 2013
Reimbursement contracts, in which health insurers receive rebates from drug
manufacturers instead of paying the transparent list price, are
becoming increasingly common worldwide. Through interviews with policy
makers in nine high-income countries, we describe the use of these
contracts around the globe and identify related policy challenges and
best practices. Of the nine countries surveyed, the majority routinely
use confidential reimbursement contracts. This alternative to drug
coverage at list prices offers benefits but is not without challenges.
Payers face increased administrative costs, difficulties enforcing
contracts, and reduced information about prices paid by others. Among
the best practices identified, policy makers recommend establishing
clear and consistent processes for negotiating contracts with relatively
simple rebate structures and transparency to the public about the
existence, purpose, and type of reimbursement contracts in place. Policy
makers should also work to address undesirable price disparities within
their countries and internationally, which may occur as a result of
this new pricing paradigm.
31 de març 2025
Pooling plasma, quin desastre!
Blood Farm. The Explosive Big Pharma Scandal that Altered the AIDS Crisis
Resumit amb IA
El llibre "Blood Farm " detalla la tragèdia i l'escàndol de la sang contaminada, principalment relacionada amb l'ús del Factor VIII per al tractament de l'hemofília, i la seva contaminació amb virus com el VIH (causant de la SIDA) i l'hepatitis C. El llibre explora com milers de persones amb hemofília al Regne Unit i als Estats Units van resultar infectades per aquests virus a causa de productes sanguinis contaminats, i com les empreses farmacèutiques, els metges i els governs van gestionar la crisi, sovint amb negligència i encobriment.
El llibre presenta diverses perspectives i línies argumentals:
- Els orígens i la naturalesa del problema: El Factor VIII, derivat de plasma sanguini de múltiples donants, es va convertir en un tractament revolucionari per a l'hemofília. No obstant això, el procés de "pooling" de plasma de milers de donants va fer que una sola donació infectada pogués contaminar lots sencers de producte. La falta de proves de detecció viral adequades i la lentitud en l'adopció de processos d'inactivació viral, com el tractament tèrmic, van agreujar el problema.
- La propagació de la informació i la reacció inicial: A principis dels anys 80, van començar a sorgir informes sobre una possible "malaltia misteriosa" (SIDA) que afectava persones amb hemofília que havien rebut productes sanguinis nord-americans. Tot i les advertències i les evidències creixents sobre el risc de transmissió del VIH i l'hepatitis a través del Factor VIII importat dels EUA, les autoritats sanitàries del Regne Unit van ser lentes a reaccionar i a advertir adequadament els pacients.
- El paper de les institucions i els individus clau:
- Treloar's School: El llibre explora el cas de Treloar's, una escola per a nens amb discapacitats físiques on molts estudiants amb hemofília van ser tractats amb Factor VIII contaminat i potencialment utilitzats en assaigs clínics sense consentiment informat. El doctor Aronstam, responsable del centre d'hemofília de l'escola, va tenir un paper central en el tractament dels nens i en la recopilació de dades.
- Doctors i hematòlegs: Figures com el Professor Bloom a Cardiff van començar a reconèixer el vincle entre el Factor VIII i la SIDA. Tot i algunes veus que alertaven sobre els riscos, hi va haver una reticència inicial per part de la comunitat mèdica i les autoritats a acceptar i comunicar la magnitud del problema.
- Pacients i famílies: El llibre narra les històries personals de pacients com Ade i Bryan, que van resultar infectats amb VIH a través del tractament amb Factor VIII. També es destaca la lluita de famílies com els Cross per buscar justícia per la infecció del seu fill Brad.
- Advocats i activistes: Tom Mull, un advocat, va tenir un paper crucial en la investigació i la presentació de demandes contra les companyies farmacèutiques als EUA. Activistes com Dana Kuhn van treballar per exposar la veritat i buscar responsabilitats.
- Periodistes: Sue Douglas del Mail on Sunday va ser una de les primeres a portar la història de la "sang assassina" a l'atenció pública al Regne Unit.
- La resposta de les companyies farmacèutiques: El llibre exposa com companyies com Alpha, Armour, Baxter i Bayer van continuar venent Factor VIII potencialment contaminat fins i tot quan van sorgir proves dels riscos. Es detallen pràctiques com la recollida de plasma en presons (incloent Angola a Louisiana) i d'altres fonts d'alt risc, i la continuació de la venda de productes no tractats tèrmicament quan ja hi havia alternatives més segures disponibles. També es revela com algunes companyies van prioritzar els beneficis econòmics per sobre de la seguretat dels pacients, fins i tot intentant encobrir els riscos.
- Les batalles legals i la recerca de justícia: El llibre segueix les complexes batalles legals als Estats Units, com el cas de la família Cross contra Cutter, on les companyies van intentar negar la seva responsabilitat. També es menciona la situació a França i al Canadà, on es van prendre mesures diferents.
- La investigació i les revelacions posteriors: El llibre fa referència a la Infected Blood Inquiry al Regne Unit, una investigació pública exhaustiva que va començar molts anys després per examinar a fons l'escàndol i les responsabilitats. Es destaca la importància de documents interns de les companyies i del govern que van ser descoberts i que revelaven el coneixement que tenien dels riscos i la seva resposta.
- L'impacte a llarg termini i la recerca de tancament: El llibre explora les conseqüències devastadores per a les persones infectades i les seves famílies, incloent la malaltia, l'estigma i la mort. També es reflexiona sobre la dificultat de trobar un tancament per a aquesta tragèdia i la importància que es faci justícia i s'aprenguin les lliçons per al futur.
En resum, "Blood Farm" és una investigació profunda i emotiva sobre un dels pitjors desastres sanitaris de la història, que revela la negligència, l'avarícia i l'encobriment que van portar a la infecció de milers de persones amb hemofília, i la llarga i difícil lluita per la veritat i la justícia per part de les víctimes i les seves famílies.

PS. Avui, Gutierrez-Rubí a LV, encertat

PS. I en Miguel Hernán

02 d’octubre 2014
Fasten seat belts
We have entered into an unknown new world: drug prices -for innovative drugs- are on track to disappear. The NHS has agreed a cap on expenditure for a hepatitis C (sofobusvir) new drug in €125m without disclosing the unit price. Some people may consider it an opaque strategy in times that politicians claim transparency.
In my opinion, such a situation allows to understand better that the pharmaceutical market for innovative drugs is mostly a monopsony (one buyer) in a monopoly (one seller), it is not a competitive market - and this is what I have always considered. Therefore, resource allocation is the result of a bargaining between both parties, and the unit price is irrelevant. The buyer wants to maximize health, the seller is maximizing income, this is exactly the struggle.
The key question is: How much is NHS willing to pay for better health?. As far as the budget is limited, the number of treatments times the price is not the right way to proceed to maximize health under constrained resources.
Any government has to set priorities for expenditure according to expected health value created. This information should be public. In any case, when a new drug is available the government should clearly define which benefits are cancelled and which are acceptable. A responsible minister can't agree new expenditures without any budget.
Therefore, innovative pharmaceutical market is not really a market -right now is clear- and governments should set priorities according to resources available -right now is also clear that they haven't done it-.
Fasten seat belts, we are entering into trying times without any political compass-gps. Citizens are expecting something different. I still remember when Victor Fuchs told long time ago: usually health economists discuss incremental cost-effectiveness in limited marginal terms, the real issue appears when such an amount is enormous. The case of hepatitis C is the example of such a situation, and only health policy and deliberative democracy are the tools to confront it. Unfortunately, this was not the strategy applied nearby.
PS. Catalonia in contention, at Harvard Political Review. Must read, if you are interested on what's going on. Otherwise, try Bloomberg op-ed or LAtimes.
PS. Reading Francesc-Marc Alvaro op-ed I always learn something.
PS. Rating catalans' well-being by OECD.

In my opinion, such a situation allows to understand better that the pharmaceutical market for innovative drugs is mostly a monopsony (one buyer) in a monopoly (one seller), it is not a competitive market - and this is what I have always considered. Therefore, resource allocation is the result of a bargaining between both parties, and the unit price is irrelevant. The buyer wants to maximize health, the seller is maximizing income, this is exactly the struggle.
The key question is: How much is NHS willing to pay for better health?. As far as the budget is limited, the number of treatments times the price is not the right way to proceed to maximize health under constrained resources.
Any government has to set priorities for expenditure according to expected health value created. This information should be public. In any case, when a new drug is available the government should clearly define which benefits are cancelled and which are acceptable. A responsible minister can't agree new expenditures without any budget.
Therefore, innovative pharmaceutical market is not really a market -right now is clear- and governments should set priorities according to resources available -right now is also clear that they haven't done it-.
Fasten seat belts, we are entering into trying times without any political compass-gps. Citizens are expecting something different. I still remember when Victor Fuchs told long time ago: usually health economists discuss incremental cost-effectiveness in limited marginal terms, the real issue appears when such an amount is enormous. The case of hepatitis C is the example of such a situation, and only health policy and deliberative democracy are the tools to confront it. Unfortunately, this was not the strategy applied nearby.
PS. Catalonia in contention, at Harvard Political Review. Must read, if you are interested on what's going on. Otherwise, try Bloomberg op-ed or LAtimes.
PS. Reading Francesc-Marc Alvaro op-ed I always learn something.
PS. Rating catalans' well-being by OECD.

Ricard Molina. Muntaner-Velódromo. Galeria Barnadas
03 de novembre 2024
La gestió de la innovació a les ciències de la vida
Managing Discovery in the Life Sciences
Aquest llibre explora els factors clau que impulsen la invenció en les ciències biomèdiques, centrant-se en com els descobriments es transformen en productes comercialitzables.
El llibre s'estructura al voltant de tres preguntes fonamentals: Quins incentius o recompenses van impulsar el descobriment? D'on provenien els recursos per a la investigació i el descobridor? Com es va traduir el descobriment en un producte comercialitzable?
El llibre analitza diversos casos d'estudi que mostren els diversos camins i graus d'èxit en el procés de descobriment i comercialització.
S'hi inclouen exemples com els estatines (inhibidors de la síntesi del colesterol), els inhibidors de l'ECA (utilitzats per tractar la hipertensió), l'angioplàstia (un procediment per obrir artèries bloquejades), el tractament de l'hepatitis C, la recerca de tractaments per a la malaltia d'Alzheimer [2] i la història de la metformina (un medicament per a la diabetis).
El llibre també examina la importància de l'estructura organitzativa per fomentar descobriments comercialitzables. Analitza com els incentius, l'assignació de recursos i la creació de cultures innovadores influeixen en la productivitat i la creativitat en la recerca.
Finalment, el llibre es pregunta si les polítiques públiques podrien millorar el procés de gestió dels descobriments biomèdics per beneficiar la societat.
A més a més, el llibre busca desmentir les crítiques infundades dirigides a la indústria biomèdica, especialment a la indústria farmacèutica, posant de manifest els beneficis que ha aportat a la societat a través dels seus descobriments i medicaments.
El llibre conclou amb una crida a la reflexió sobre com podem augmentar el flux de nous productes sense incrementar els costos de R+D. S'interroga sobre la millor manera d'assignar els fons de recerca bàsica i de traduir els descobriments en productes comercialitzables de forma més ràpida i econòmica.

Resum amb IA
El llibre "Managing Discovery in the Life Sciences: Harnessing Creativity to Drive Biomedical Innovation" (2018), escrit pels acadèmics Philip A. Rea, Mark V. Pauly i Lawton R. Burns, és una anàlisi interdisciplinària (bioquímica, economia i sociologia) sobre com s'originen i es gestionen els descobriments biomèdics per arribar al mercat.
1. El marc dels tres pilars
L'obra utilitza un esquema organitzatiu basat en tres preguntes fonamentals que s'apliquen a cada cas d'estudi:
- L'incentiu o recompensa: Què va motivar l'inventor a ser el primer a fer el descobriment (ja sigui fama, altruisme o benefici financer)?.
- Els recursos: D'on van provenir els mitjans econòmics i humans per cobrir el procés de recerca (suport públic, capital privat o inversió filantròpica)?.
- La traducció al mercat: Com es va convertir un coneixement científic bàsic en un producte o procés que es pot vendre i utilitzar clínicament?.
2. Teoria econòmica i desmitificació
Els autors dediquen els primers capítols a analitzar l'economia del sector farmacèutic, desmuntant diversos mites:
- El model de Ricardo: Argumenten que l'augment dels costos de R+D no es deu necessàriament a la ineficiència, sinó al fet que l'augment de la demanda i el valor de la salut fan que sigui rendible per a les empreses investigar oportunitats "menys fèrtils" o més difícils que abans s'haurien descartat.
- Preus i R+D: Subratllen que, des d'un punt de vista econòmic racional, el preu d'un medicament no depèn dels costos de R+D ja invertits, sinó de la voluntat de pagament del mercat i de l'elasticitat de la demanda.
3. Estudis de cas significatius
El nucli del llibre són 11 casos d'estudi que il·lustren la complexitat del procés:
- Les estatines: Mostra com el descobriment d'un científic japonès (Akira Endo) en fongs va ser transformat per gegants com Merck i Pfizer en un tractament massiu per al colesterol, gràcies a la intuïció científica i la gestió de riscos.
- La metformina: Un exemple de "descobriment per error i atzar" que prové del folklore medieval (la ruda de cabra) i que va trigar dècades a ser aprovat als EUA a causa de prejudicis sobre medicaments similars que havien fallat.
- Gleevec: Representa el triomf de la teràpia de precisió, on el coneixement de la causa molecular del càncer (el cromosoma Filadèlfia) va permetre dissenyar un medicament que bloqueja específicament la divisió de les cèl·lules leucèmiques.
- Hepatitis C: Narra la cursa per trobar una cura totalment oral i sense interferó, destacant la importància de les adquisicions d'empreses biotecnològiques (com la compra de Pharmasset per part de Gilead).
4. Gestió i organització de la innovació
Els autors analitzen com les estructures organitzatives afecten la creativitat:
- Ecosistemes de diversos nivells: El descobriment té lloc en un entorn que inclou l'individu, l'equip, l'empresa i clústers geogràfics com Cambridge (MA) o San Diego (CA).
- "Wild Ducks" i "Black Sheep": S'emfatitza que les empreses innovadores han de reclutar i tolerar individus dissidents o no conformistes que tenen la passió de persistir on altres fallen.
- Resiliència i Agilitat: El cas de Regeneron il·lustra una empresa dirigida per científics que va sobreviure a fracassos inicials mantenint la seva estabilitat directiva i pivotant cap a noves plataformes tecnològiques.
5. El paper del govern i el futur
El llibre conclou que el govern té un paper limitat però crucial:
- Límits de la gestió pública: Tot i que el NIH i el finançament públic són vitals per a la ciència bàsica, la seva productivitat en termes de nous fàrmacs comercialitzables és relativament baixa en comparació amb el sector privat.
- Importància de la serendipitat: Es recorda que el descobriment és intrínsecament "salvatge" i impredictible; per tant, les polítiques han de ser permissives i fomentar múltiples models de col·laboració en lloc d'intentar centralitzar la innovació mitjançant una planificació burocràtica rígida.
En resum, el llibre defensa que l'èxit en les ciències de la vida no prové d'un sol geni ni d'un procés lineal, sinó d'una combinació de ciència rigorosa, determinació personal, serendipitat i un entorn econòmic que permeti capturar els retorns de la innovació.
21 d’agost 2025
Pharma, big pharma (43)
The Valeant scandal. Inside the Enron of pharma
L'informe detalla el cas de Valeant Pharmaceuticals International, posteriorment reanomenada Bausch Health Companies, com un exemple destacat de frau comptable a la indústria farmacèutica, comparant-lo amb Enron.
Aquí teniu un resum detallat:
1. Ascens i caiguda de Valeant
- Ascens meteòric: Valeant va ser una de les accions amb millor rendiment als EUA durant els cinc anys fins a l'agost de 2015, amb un guany acumulat de gairebé el 1.800%, aspirant a ser l'empresa farmacèutica més gran d'Amèrica.
- Investigació i col·lapse: Al quart trimestre de 2015, la SEC va anunciar una investigació sobre les pràctiques comptables de la companyia, provocant una caiguda catastròfica del 90% en el preu de les accions, de la qual mai no s'ha recuperat.
- Càrrecs formals: La SEC va acusar formalment Valeant el juliol de 2020 per pràctiques comptables inadequades, i l'empresa no ha registrat beneficis des del 2018.
- Similituds amb Enron: Es compara freqüentment amb "l'Enron de la Farmàcia" per similituds com, ser estimades per Wall Street, ser dirigides per antics consultors de McKinsey, reportar un creixement explosiu, utilitzar entitats arm's-length per falsejar ingressos i col·lapsar després de ser investigades per frau comptable, tot i que l'escala del frau no va ser comparable.
2. Detecció de Transparently.AI
- Advertències prèvies: Molts analistes i inversors es van sorprendre per la caiguda de Valeant, però el sistema Transparently va classificar constantment Valeant en el 5% al 15% inferior de totes les empreses a nivell mundial per la seva qualitat comptable durant la dècada anterior a la investigació de la SEC.
- Robustesa del sistema: La capacitat del sistema d'IA de Transparently per detectar manipulacions a Valeant és notable, considerant la dificultat d'analitzar financerament les empreses farmacèutiques a causa de factors com la gran dependència de R+D, la valoració subjectiva de fàrmacs, les diferències de preus entre jurisdiccions, els esquemes de preus complexos i la diversitat de canals de distribució.
3. Valeant sota Milan Panić (1959-2002)
- Orígens i lideratge: La companyia va ser fundada el 1959 com ICN Pharmaceuticals Corporation (ICN) per Milan Panić, un líder "colorista i enèrgic" que la va dirigir durant 42 anys, excepte un període en què va servir com a Primer Ministre de Iugoslàvia.
- Creixement i adquisicions: ICN va créixer a través de la investigació de fàrmacs i l'adquisició d'empreses farmacèutiques barates en àrees de nínxol, superant els 100 milions de dòlars en vendes a principis dels anys 70.
- Medicaments clau i controvèrsies inicials:
- L-dopa: Aprovació el 1970 per a la malaltia de Parkinson, però l'acció va caure bruscament per efectes secundaris greus.
- Ribavirin (Virazole): Sintetitzat el 1970, ICN va afirmar que seria eficaç contra un ampli espectre de virus. Tot i les dificultats d'aprovació per part de la FDA, degut a la complexitat dels antivirals. La patent d'un fàrmac sol durar 20 anys des de la creació, però el desenvolupament i l'aprovació poden consumir 10-12 anys, deixant només 8-10 anys de vida productiva.
- Primeres investigacions de la SEC (1977): La SEC va presentar una queixa contra ICN i Panić per violacions de la Llei de Borsa de Valors de 1934, al·legant manipulació de valors (incloent-hi ús d'informació privilegiada) i informes financers falsos mitjançant afirmacions de fàrmacs exagerades. Van acordar abstenir-se de futures violacions sense admetre cap delicte.
- Aprovació limitada de Ribavirin (1985): Finalment aprovat només per al virus respiratori sincitial (RSV), ICN va ser obligada a retirar un comunicat de premsa per afirmacions falses o enganyoses sobre l'eficàcia i la minimització dels efectes secundaris. Tot i això, ja el venien en països amb regulacions menys estrictes.
- Controvèrsies amb Ribavirin per a l'AIDS (1986-1989):
- ICN va anunciar que el Virazole "podria retardar l'aparició de la SIDA".
- Una oferta d'accions i bons de PaineWebber va provocar una pujada del 67% en l'acció, seguida de demandes per inflar el preu i investigacions de la SEC per ús d'informació privilegiada.
- Panić també va ser demandat per l'IRS i per impagament de préstecs.
- Finalment, ICN va abandonar els esforços d'aprovació per a la SIDA, va registrar una pèrdua de 82 milions de dòlars el 1989, però va atorgar augments salarials "monumentals" als seus directius, incloent-hi Panić.
- Acords legals: El 1991, ICN va pagar 600.000 dòlars per càrrecs de la FDA per tergiversar les propietats medicinals de ribavirin, i un acord amb la SEC. Una demanda col·lectiva es va resoldre el 1996 amb 14,5 milions de dòlars en danys.
- Política a Iugoslàvia: Panić va adquirir el 75% de Galenika Pharmaceutical i va expandir ICN a l'Europa de l'Est. Va servir com a Primer Ministre de Iugoslàvia (juliol 1992-març 1993), però va perdre les eleccions presidencials "manipulades" i el govern iugoslau va renegar dels pagaments, causant grans pèrdues a ICN, mentre Panić rebia un sou i una bonificació considerables com a CEO absent.
- Rebrot de Ribavirin per a l'Hepatitis C: Després de la seva aventura iugoslava, Panić va tornar a centrar-se en ribavirin per a l'Hepatitis C. La FDA va rebutjar l'aplicació d'ICN el novembre de 1994, una notícia material que la companyia va trigar tres mesos a revelar, provocant una caiguda del 41% en l'acció.
- Nou cas d'ús d'informació privilegiada: Panić va vendre 55.000 accions per 1,24 milions de dòlars l'endemà de la carta de rebuig de la FDA, provocant una altra investigació de la SEC i una demanda col·lectiva. ICN va realitzar una revisió interna que va exonerar Panić.
- Adquisicions de nínxol i èxits comercials: Tot i els problemes legals, ICN va continuar amb adquisicions de nínxol, arribant a vendes anuals superiors als 500 milions de dòlars el 1996 amb distribució en més de 60 països. Ribavirin, tot i estar aprovat només per a RSV als EUA, s'aprovava en més de 40 països per a diverses infeccions virals, representant el 10% de les vendes d'ICN i una part "molt més gran" dels beneficis per royalties.
- Més acords i la caiguda final de Panić: El 1997, la companyia va pagar 15 milions de dòlars per resoldre la demanda col·lectiva per la venda d'accions de Panić. El 1998, la SEC va abandonar la seva investigació per ús d'informació privilegiada, però va presentar una demanda civil per no revelar oportunament el rebuig de la FDA. El 2001, ICN es va declarar culpable d'un càrrec de frau de valors criminal i va pagar 5,6 milions de dòlars en multes. El 2002, la SEC va tancar la seva acció civil, amb ICN pagant un altre milió de dòlars i Panić 500.000 dòlars en sancions civils. Aquestes pèrdues legals van fer inevitable la seva destitució el 12 de juny de 2002. La companyia va canviar el seu nom a Valeant per distanciar-se de l'era Panić.
- Qualitat comptable sota Panić: Entre 1999 i 2003, el sistema Transparently va classificar ICN en el 5% inferior de les empreses del sector sanitari dels EUA per la qualitat i transparència comptable.
- El 1999, ICN tenia una puntuació de risc de manipulació comptable del 77%, considerada "molt pobra" per una empresa d'aquella capitalització i sota investigació.
- Es van detectar senyals d'alarma en 10 dels 14 grups de risc, incloent-hi senyals de creixement, capital circulant, crèdit i qualitat d'actius.
- Les dades van mostrar patrons consistents amb esforços per inflar vendes i guanys, a més de signes de tensió financera.
- Alertes principals (1999): Comptes a pagar molt allargats (dificultat de pagament), creixement d'actius molt superior al de vendes (adquisicions o disfressa de despeses operatives com inversió), qualitat d'actius sospitosa (grans intangibles, capitalització agressiva de despeses operatives), comptes a cobrar extremadament volàtils (manipulació de vendes), i preocupacions de crèdit (creixement de vendes anormalment feble en relació amb el creixement d'actius, baix palanquejament en relació amb la capitalització de mercat, despeses d'interessos volàtils, ús de finançament derivat car i dilutiu).
- La puntuació de risc no es va dominar per factors típicament associats amb empreses farmacèutiques, sinó per mesures relacionades amb el reconeixement inadequat d'ingressos.
4. Valeant sota Michael Pearson (2008-2016)
- Nou enfocament estratègic: Després de la marxa de Panić, la companyia va canviar el nom a Valeant i es va centrar en la reducció de costos i adquisicions, principalment en dermatologia i cosmètica. La venda de la unitat de R+D va deixar la companyia sense una cartera de fàrmacs significativa.
- Pearson al capdavant (2008): Michael Pearson, un veterà de McKinsey i expert en adquisicions farmacèutiques, va ser nomenat CEO. Pearson creia que l'adquisició era l'únic camí segur per generar valor per a l'accionista, mentre que el desenvolupament de fàrmacs patentats era "una tonteria".
- Model de negoci basat en M&A: Valeant es va convertir en un "juggernaut" d'M&A, amb una "set insaciable" de negocis finançats amb deute i enginyeria financera complexa, reduint la despesa en R+D a només el 6% de les vendes (enfront del 18% de mitjana de la indústria).
- Aquesta estratègia era insostenible, ja que les adquisicions rares vegades amortitzaven la inversió en menys de cinc anys, i requeria un creixement exponencial del deute per sostenir els guanys, a menys que Valeant pogués compensar la decadència dels preus dels fàrmacs que perdien la patent o "simplement mentís" sobre els seus guanys.
- Èxit inicial i la "bombolla": A finals de 2008, l'acció de Valeant es cotitzava a 9,65 dòlars; el juliol de 2015, va assolir un màxim de 236,10 dòlars, un retorn de més del 2.200%.
- Fusió inversa amb Biovail (2010): Biovail, la farmacèutica canadenca, va adquirir Valeant mitjançant una "inversió corporativa". Pearson va seguir sent CEO, l'entitat combinada va prendre el nom i l'estratègia de Valeant, però es va incorporar al Canadà, reduint la seva taxa impositiva efectiva del 35% al 15%. L'acord va augmentar el deute a llarg termini en 3.200 milions de dòlars.
- L'historial fosc de Biovail: Biovail havia pagat 138 milions de dòlars el 2007 per resoldre una demanda per falsejar declaracions per inflar el preu de les accions, i el 2008 la SEC va acusar la companyia i els seus ex-executius de frau comptable. La col·laboració amb Biovail va ser un "enorme senyal d'alarma" sobre l'ètica de govern de Valeant.
- Estratègia de preus abusius: Pearson buscava empreses amb fàrmacs subestimats, sovint fàrmacs essencials per a malalties cròniques amb patents que encara no havien expirat.
- A mesura que l'estratègia d'adquisicions es feia més difícil i els costos del deute augmentaven, els augments de preus es van fer més extrems. El 2014, la companyia va augmentar els preus de 62 fàrmacs una mitjana del 50%. L'any següent, 56 medicaments van tenir augments d'una mitjana del 65,6%, i alguns van superar el 500%.
- El maig de 2015, el CFO va admetre que els augments de preus representaven al voltant del 80% del creixement dels ingressos.
- Escrutini regulador i polític: Aquestes pràctiques van cridar l'atenció de congressistes i fiscals. L'octubre de 2015, Valeant va ser citada per fiscals buscant detalls sobre programes d'assistència al pacient, preus de fàrmacs i pràctiques de distribució.
- La relació amb Philidor: El New York Times va revelar com Valeant utilitzava els seus vincles amb la farmàcia especialitzada Philidor per vendre medicaments convencionals. Més tard es va revelar que Valeant havia ajudat a establir, finançar i subvencionar Philidor, pagant 100 milions de dòlars per una opció de compra per 1 dòlar, convertint Philidor en una Entitat d'Interès Variable (VIE) controlada per Valeant, i els seus resultats ja estaven incorporats en els de Valeant.
- Caiguda de l'acció i Pearson's sortida: Entre l'agost de 2015 i el febrer de 2016, les accions de Valeant van perdre més del 60% del seu valor. El febrer de 2016, Valeant va revelar que estava sota investigació de la SEC, i el març, Pearson va anunciar la seva marxa, i la companyia va admetre problemes comptables i "conducta impròpia" per part d'alts executius financers.
5. Investigació de Philidor i càrrecs de la SEC
- Nou lideratge: El maig de 2016, Joseph Papa va reemplaçar Pearson com a CEO, i la companyia va ser reanomenada Bausch Health Inc. La prioritat principal era reduir el deute de 30 milions de dòlars acumulat.
- Rol de Philidor en el frau: La investigació criminal de Philidor va determinar que la farmàcia alterava receptes amb la intenció d'omplir més receptes amb medicaments de marca Valeant, aconseguint que les companyies d'assegurances paguessin per fàrmacs costosos mentre Philidor "simulava ser neutral".
- Sentències criminals: El CEO de Philidor i un executiu de Valeant van ser empresonats per un esquema de comissions il·legals.
- Sanció de la SEC (2020): El 31 de juliol de 2020, la SEC va anunciar que Bausch Health pagaria una penalització de 45 milions de dòlars per resoldre els càrrecs de reconeixement d'ingressos inadequat i divulgacions enganyoses. L'ex-CEO, CFO i controlador també van acceptar pagar multes.
- Irregularitats comptables: Valeant havia falsejat transaccions d'ingressos i inclòs assignacions d'ingressos errònies. En particular, va informar un creixement de dos dígits en les vendes de la mateixa botiga durant cinc trimestres consecutius, derivades de Philidor, sense revelar la seva relació "única" o els riscos associats a Philidor.
- A més, Valeant no va revelar l'impacte material dels ingressos rebuts dels majoristes de fàrmacs després d'un augment del 500% del preu d'un sol fàrmac, atribuint erròniament els ingressos a més de 100 productes no relacionats.
6. Qualitat comptable sota Pearson
- Persistent risc comptable: La puntuació de risc de manipulació comptable de Valeant, segons Transparently, va millorar lleugerament el 2009 (comú amb nous CEOs), però a partir del 2010 va tornar als nivells de l'era Panić, situant-se en el 5% inferior de les empreses a nivell mundial per la qualitat i transparència comptable.
- Canvi en els riscos: El model de negoci basat en l'adquisició va desplaçar els riscos comptables cap a preocupacions sobre el palancament i la sostenibilitat, i lluny de la tensió financera relacionada amb la generació de caixa i problemes de crèdit. Això es deu al fet que l'obtenció de milers de milions de deute tendeix a resoldre els problemes de caixa immediats.
- Noves alertes (2013):
- Major palanquejament: El ràtio de deute a capital de Valeant era 18 vegades superior a la mitjana global de les empreses sanitàries.
- Suavització de guanys més agressiva: La companyia semblava utilitzar acumulacions per inflar els guanys, possiblement a causa de la pressió per complir els objectius d'ingressos trimestrals i la seva alta valoració de mercat.
- Qualitat d'ingressos i marges: Una part significativa dels ingressos derivava d'activitats no operatives, indicant que les operacions principals podrien no ser suficients per sostenir el negoci, i es registraven càrrecs extraordinaris significatius.
- Profitabilitat anormal: Malgrat l'aparentment bon EBITDA i els marges operatius, el sistema va veure la "profitabilitat anormal" de Valeant en una indústria establerta com un senyal de inflació artificial d'ingressos o un model que avançava els guanys a curt termini a costa dels futurs, posant en dubte la sostenibilitat del negoci.
- Conclusió del sistema Transparently: El sistema va fer sonar les alarmes sobre Valeant durant tot el mandat de Pearson, advertint sobre la sostenibilitat del model de negoci i el risc d'ingressos falsejats. Per a una empresa amb una puntuació de risc comptable tan pobra, era "típicament només qüestió de temps abans que la SEC actués".

08 de juny 2025
El mercat farmacèutic tensionat
Economic Markets and Pharmaceutical Innovation
Aquí teniu un resum detallat de l'article "Economic Markets and Pharmaceutical Innovation" de Craig Garthwaite, basant-me en la informació proporcionada a les fonts:
L'article, publicat al Journal of Economic Perspectives, ofereix un resum ampli del coneixement existent sobre diversos aspectes econòmics importants del mercat farmacèutic relacionats amb el procés innovador. L'autor és Craig Garthwaite, Professor d'Estratègia a la Kellogg School of Management de la Northwestern University. L'objectiu és ajudar aquells interessats o involucrats en debats sobre la indústria farmacèutica a entendre els fets i patrons econòmics fonamentals al voltant dels incentius per al desenvolupament de medicaments.
L'article comença assenyalant una tensió central en els mercats farmacèutics: tot i que els beneficis dels fàrmacs innovadors són poc discutits, molts pregunten raonablement "A quin preu?". Les enquestes d'opinió pública mostren una favorabilitat neta negativa per a la indústria farmacèutica, tot i que els fàrmacs innovadors han tingut un èxit enorme en el tractament i la curació de diverses condicions. Per exemple, les innovacions farmacèutiques són responsables del 35% de la notable disminució de la mortalitat cardiovascular del 1990 al 2015. Condicions prèviament mortals com el VIH/SIDA s'han transformat en malalties cròniques manejables, i l'hepatitis C s'ha curat. Teràpies gèniques i avanços en immuno-oncologia estan proporcionant millores significatives. Recentment, han aparegut tractaments efectius per a l'obesitat (agonistes GLP-1) amb millores en resultats cardiometabòlics.
Els preus elevats dels medicaments de marca innovadors no són accidentals, sinó el resultat de polítiques destinades a proporcionar incentius financers per al desenvolupament continu de nous productes. Aquestes polítiques són necessàries a causa d'una fallada de mercat intrínseca a la innovació farmacèutica. Les empreses que desenvolupen productes nous creen béns públics en forma de coneixement científic. Un cop desenvolupat aquest coneixement, és relativament fàcil per a una altra empresa replicar el producte a un cost fix molt menor i reduir el rendiment financer per a l'innovador original. Per tant, sense protecció de la propietat intel·lectual, poques empreses racionals invertirien els grans costos i riscos necessaris per a la innovació, especialment amb llargs períodes de retorn i baixos costos d'imitació. El sistema actual implica que els governs proporcionin protecció de la propietat intel·lectual per períodes limitats, permetent a les empreses innovadores vendre els seus productes a un preu més alt sense competència directa.
Aquesta protecció de la propietat intel·lectual crea un equilibri entre accés a curt termini i incentius a llarg termini. Els preus elevats redueixen l'accés a les innovacions existents a curt termini, cosa que pot tenir conseqüències devastadores per als pacients. Tanmateix, aquests preus elevats proporcionen incentius financers per a futures inversions en el desenvolupament de nous productes, que podrien resoldre la manca de tractaments per a condicions que actualment no en tenen.
El desenvolupament de productes farmacèutics innovadors requereix inversions grans, fixes i enfonsades en R&D (recerca i desenvolupament). Aquests fons provenen d'empreses privades, universitats i institucions públiques. Molts productes exitosos comencen en laboratoris acadèmics i petites firmes de biotecnologia. La inversió del sector privat en R&D farmacèutic va ser de 276.000 milions de dòlars a nivell mundial el 2021.
Nombrosos estudis empírics mostren una relació entre la mida esperada del mercat d'un fàrmac i la magnitud de les inversions en R&D. Les firmes responen a la mida econòmica potencial del mercat d'un producte, no només al nombre de pacients potencials. Per exemple, l'expansió de Medicaid als EUA va tenir un augment modest en els ingressos a causa dels preus més baixos que paga Medicaid, i no va resultar en un augment de les inversions en R&D. Les tàctiques de negociació més fortes, com l'exclusió de cobertura, van reduir el retorn financer per pacient potencial i van disminuir les inversions en R&D en àrees amb substituts terapèutics competidors. La diferència de preus entre els EUA i altres mercats desenvolupats suggereix que molts altres mercats són probablement massa petits per ser determinants en les decisions d'inversió en desenvolupament de fàrmacs de les firmes innovadores, cosa que explica per què poden negociar preus molt més baixos sense grans temors de reduir la innovació futura.
El benefici exacte creat per aquestes inversions incrementals en R&D no està clar. La quantitat de despesa en R&D o el nombre de productes nous són mètriques incompletes del benefici social. Els estudis sobre la novetat científica dels fàrmacs marginals donen resultats contradictoris. Alguns estudis suggereixen que els augments de la mida del mercat per polítiques com Medicare Part D van portar a productes que no eren científicament nous en el seu enfocament bàsic, sinó noves combinacions d'enfocaments existents. Altres troben que les firmes amb grans infusions de caixa per polítiques com Medicare Part D van augmentar les inversions en productes més científicament nous, independentment dels retorns potencials, suggerint que les infusions de caixa van reduir les friccions en el mercat financer. Aquests resultats suggereixen que promoure la innovació més científica pot requerir abordar impediments específics com l'aversió al risc o la manca de ciència bàsica. La novetat científica no és suficient per encapsular els efectes del benestar dels nous productes; les noves aplicacions de mecanismes d'acció existents també poden tenir impactes significatius en la salut i el benestar econòmic.
La determinació dels ingressos potencials per a un nou producte farmacèutic depèn de qui és el client, quin és exactament el "preu" i la mida esperada del mercat. Això requereix comprendre el mecanisme d'establiment de preus, els determinants de la demanda i els factors institucionals que els influeixen.
La cadena de valor farmacèutica implica tres tasques perquè una innovació tingui èxit comercial: (1) aprovació per un regulador, (2) acceptació de pagament per un tercer pagador, i (3) adopció per part dels clínics i pacients.
Hi ha dues cadenes de valor principals:
- Fàrmacs al detall ("retail pharmaceuticals"): Prescrits per un metge i comprats a una farmàcia. La relació entre els tercers pagadors (asseguradores), les firmes gestores de beneficis farmacèutics ("pharmacy benefit managers" o PBMs) que contracten, i els fabricants de medicaments és crucial. Els productes entren amb un preu de llista ("list price"). El PBM negocia un descompte amb el fabricant, conegut com a "rebate" (rebaixa), que varia segons el poder de negociació. Els rebaixes es mantenen confidencials per facilitar descomptes més grans. Els PBMs i els fabricants també negocien la gestió de la utilització, on majors descomptes resulten en menys eines com autoritzacions prèvies o teràpia esglaonada. La gestió de la utilització també pot incloure eines financeres com deduccibles, coassegurança i copagaments. Els PBMs obtenen ingressos de quotes per membre per mes, un percentatge de la rebaixa negociada i el diferencial entre el que paguen a la farmàcia i el que el patrocinador del pla els paga ("spread pricing"). La compensació dels PBMs, especialment lligada a les rebaixes, genera controvèrsia.
- Fàrmacs administrats per metges ("physician-administered drugs"): Sovint són productes biològics administrats en un consultori mèdic. Aquests es paguen sota la porció "mèdica" del benefici de l'assegurança i no involucren PBMs. Els proveïdors sanitaris els adquireixen, emmagatzemen i administren. Se'ls sol pagar un marge sobre el preu mitjà de venda del producte. A Medicare, els metges reben el 106% del preu mitjà de venda, mentre que els mercats privats solen tenir marges més grans. Aquesta forma de pagament pot distorsionar l'entrada i la difusió de nous productes, ja que els metges reben més ingressos per prescriure productes de major preu. Això ha estat una preocupació política per als incentius al desenvolupament de biosimilars. Els proveïdors més grans poden negociar descomptes més grans, cosa que pot influir en les decisions de consolidació de les firmes. Aquesta cadena de valor també pot generar distorsions, ja que les decisions de cobertura d'un pagador poden influir en la disponibilitat del fàrmac per a pacients coberts per altres pagadors.
Les negociacions determinen el preu capturat pels fabricants. Les rebaixes han crescut en magnitud i importància estratègica. L'escletxa entre el preu de llista i el preu net per a fàrmacs al detall es va mantenir relativament estable del 2009 al 2013, però després el preu de llista va escalar ràpidament mentre que el preu net va romandre constant. El 2019, la magnitud de les rebaixes es va duplicar i la mitjana era aproximadament del 53%. El preu de llista i la rebaixa depenen de l'entorn competitiu. Teràpies relativament úniques tenen preus nets més alts que s'apropen més als preus de llista. L'entrada de productes competidors, com va passar amb els tractaments per a l'hepatitis C, pot portar a fortes negociacions i disminucions de preus. L'entrada de nous productes pot estendre's més enllà de l'augment de la competència; les segones i terceres generacions de fàrmacs poden proporcionar una eficàcia superior, menys efectes secundaris o ser millors per a grups de pacients específics. En aquests casos, els preus no cauen amb l'entrada, sinó que cada versió del fàrmac tracta una població més petita i específica.
Entendre la disposició a pagar ("willingness-to-pay") per als productes farmacèutics és complex. El guany en salut és un punt de partida lògic, sovint quantificat mitjançant anys de vida ajustats per qualitat (QALYs). Tanmateix, en un mercat amb assegurances, el consum es finança amb recursos de tot el grup de risc, molts dels quals no es beneficien directament de la transacció. Hi ha altres fonts potencials de valor que van més enllà del benefici directe per al pacient, com el valor d'opció per a pacients no afectats, el valor del progrés científic per a tractaments futurs i el valor d'assegurança de la innovació mèdica. Les innovacions mèdiques transformen el risc mèdic en risc financer per als individus. El valor d'assegurança d'una nova innovació pot superar el valor de l'assegurança de salut mateixa, especialment per a malalties greus amb tractaments limitats. Aquest valor d'assegurança podria explicar per què molts tractaments per a malalties rares superen els llindars basats únicament en el valor clínic. El progrés científic és iteratiu, i el valor futur creat per les innovacions futures hauria de ser tingut en compte en els ingressos dels fabricants que fan progrés incremental. Els esforços per vincular els preus dels fàrmacs al valor basat únicament en resultats clínics podrien negligir aquests altres beneficis de la innovació i crear preus artificialment baixos, alterant els incentius per invertir.
Els fabricants intenten augmentar els ingressos potencials mitjançant esforços de comercialització dirigits a pacients i proveïdors. Aquests esforços estan regulats per la FDA. Les empreses només poden publicitar per a indicacions aprovades, tot i que els metges poden utilitzar productes aprovats per a qualsevol indicació. Obtenir l'aprovació per a noves indicacions pot augmentar la informació del mercat i l'ús. Hi ha preocupacions sobre si la despesa en màrqueting és un malbaratament o un complement a la R&D; si augmenta la mida del mercat potencial, pot encoratjar la inversió en desenvolupament de productes.
El màrqueting dirigit directament als consumidors (DTC advertising) només està permès als EUA i Nova Zelanda en mercats de salut. Hi ha debat sobre si és principalment informació o persuasió. Pot informar els pacients sobre possibles tractaments, i estudis troben que pot augmentar l'ús de medicaments genèrics, cosa que seria coherent amb l'augment de visites mèdiques. D'altra banda, en una població assegurada, pacients i proveïdors podrien no ponderar adequadament el valor dels productes si no afronten el cost marginal, cosa que podria portar a l'ús de medicaments poc rendibles. Estudis han trobat que l'ús resultant del màrqueting DTC pot generar guanys per als pacients, com l'augment de l'oferta laboral o una major adherència. L'efecte sobre el benestar depèn dels beneficis clínics del fàrmac anunciat. Alguns estudis suggereixen que les firmes poden ser més propenses a anunciar fàrmacs amb menors beneficis clínics, mentre que altres troben beneficis econòmics significatius per a fàrmacs altament efectius com les estatines, superant la despesa total en publicitat DTC en el mercat.
El màrqueting dirigit als proveïdors ("detailing") implica fabricants dirigint-se als metges. La majoria dels recursos de màrqueting es dirigeixen als metges. La pregunta clau és si aquests esforços augmenten la informació disponible per als metges o només busquen influir en el seu comportament de prescripció mitjançant beneficis tangibles. Estudis suggereixen que els pagaments als metges porten a petits augments en les prescripcions i la despesa dels pacients, generant un retorn econòmicament significatiu per als fabricants. L'impacte en el benestar depèn de per què els pacients no accedien prèviament a medicacions efectives i l'eficàcia de les que acaben prenent. Alguns estudis troben que el màrqueting als metges pot augmentar l'ús tant en pacients d'alt com de baix risc d'esdeveniments adversos, generant escepticisme sobre la precisió de la informació proporcionada. Igual que amb la publicitat DTC, l'anàlisi de benestar per al detailing als metges és complex i depèn de la classe de fàrmacs. Les firmes coordinen els seus esforços de comercialització DTC i dirigits als metges.
Els incentius per a la innovació depenen que les firmes obtinguin marges positius per recuperar les inversions en R&D i regulació. Avaluar els efectes agregats requereix considerar l'impacte de les assegurances. Una assegurança que funcioni bé pot aïllar els pacients del cost directe, reduint les pèrdues de benestar per preus alts. No obstant això, estudis suggereixen que en el mercat nord-americà, altament assegurat, les quantitats de medicaments disminueixen poc després de la pèrdua de patents tot i la caiguda dels preus, indicant un grau limitat en què els preus alts limiten el consum en mercats amb assegurança. Això pot no ser cert en mercats sense assegurança o amb cost-sharing elevat. L'estructura de l'assegurança és important.
L'article descriu tres programes públics d'assegurança de medicaments:
- Medicaid: Cobreix població de baixos ingressos i discapacitada. Utilitza dos mètodes per assegurar els preus més baixos: (1) rebaixes al govern estatal de Medicaid iguals al major del 23,1% del preu de llista o la major rebaixa a qualsevol comprador comercial ("best price"), i (2) rebaixes "inflacionàries" addicionals basades en el creixement del preu de llista des del llançament del producte. Això resulta que Medicaid només paga el 35% del preu mitjà pagat per les asseguradores a Medicare Part D i el mercat comercial. Molts productes amb preus comercials alts es venen a Medicaid pràcticament sense cost. Les firmes reaccionen a aquestes polítiques; la regla del "best price" augmenta els costos per als fabricants de proporcionar descomptes al mercat comercial, actuant com un impost implícit en aquest mercat. Les rebaixes inflacionàries incentiven a limitar el creixement del preu de llista amb el temps.
- El Programa de Preus de Medicaments 340B: Creat el 1992 per subvencionar hospitals que proporcionen atenció no compensada. Permet a certs hospitals comprar productes farmacèutics aproximadament al "best price" de Medicaid. Poden vendre aquests productes a pacients ambulatoris. Quan venen a pacients de Medicaid, han d'acceptar el "best price". Per a pacients comercials o sense assegurança, poden carregar els preus que negociïn, però una gran fracció no trasllada els descomptes a pacients sense assegurança o amb poca assegurança. El programa ha crescut significativament, amb un augment enorme del nombre de farmàcies contractades i del valor dels productes. Té implicacions a nivell de mercat; en reduir els ingressos disponibles per a fàrmacs innovadors, pot disminuir els incentius per a la R&D. Té un efecte similar al de Medicaid en els preus comercials. També pot tenir altres efectes, com reduir l'incentiu a proporcionar rebaixes als plans comercials i, en alguns casos, fer que els patrocinadors dels plans paguin preus de llista més alts. El creixement del 340B s'associa amb augments en les primes d'assegurança de salut comercial. El programa està relativament poc estudiat en comparació amb altres.
- Medicare Part D: Creat el 2006 com un programa d'assegurança de medicaments al detall per a la gent gran. Està molt subvencionat pel govern, però gestionat per firmes privades que negocien preus de manera similar al mercat comercial. Històricament, incloïa un component de reassegurança ("catastrophic region") on el govern assumia la major part de la despesa un cop el pacient assolia un cert límit de despesa de butxaca. L'estructura inicial incentivava tant els plans com els fabricants a augmentar ràpidament els preus de llista, ja que això feia que els pacients de cost elevat entressin més ràpidament a la regió catastròfica coberta principalment pel govern. La Llei de Reducció de la Inflació (IRA) del 2022 va canviar l'estructura de la regió catastròfica, transferint més càrrega als patrocinadors dels plans i eliminant la porció pagada pel pacient. La IRA també va concedir autoritat a CMS per negociar preus més baixos per a fàrmacs seleccionats després de 9 anys (molècules petites) o 13 anys (biològics) de la primera aprovació. Aquest període no s'estén per noves indicacions. Les implicacions de la IRA sobre la innovació encara es debaten i són objecte d'investigació.
El cost compartit estratègic ("strategic cost sharing") en els mercats d'assegurança de medicaments implica que els pacients amb malalties cròniques que requereixen fàrmacs cars s'enfronten a un cost compartit elevat, cosa que essencialment reintrodueix la subscripció mèdica implícita. Això transfereix diners dels afiliats malalts als patrocinadors dels plans. Els fabricants han intentat disminuir l'efecte del cost compartit elevat mitjançant programes d'assistència, com els cupons de copagament ("copayment coupons"), on el fabricant paga el cost compartit en nom del consumidor. Aquests cupons estan permesos al mercat comercial, però no en programes governamentals com Medicare i Medicaid. La lògica estratègica per a les empreses és clara: un cupó actua com un descompte addicional, especialment amb coassegurances elevades. Les implicacions varien segons el tipus de competència; amb competència genèrica, els cupons poden desplaçar la quota de mercat cap a la versió de marca i augmentar els beneficis del fabricant original, sense augmentar necessàriament l'accés a la molècula. Per a productes sense substituts genèrics, els cupons augmenten el preu net (aproximadament un 8%) perquè debiliten la capacitat de l'assegurador comercial d'utilitzar el cost compartit en les negociacions, però augmenten l'accés a molècules específiques. Els PBMs i els patrocinadors dels plans intenten contrarestar aquestes estratègies, fins i tot excloent fàrmacs dels seus formularis. Els cupons no són rendibles per als fabricants si el fàrmac no està cobert. Limitar el cost compartit (com el límit per a la insulina a Medicare Part D sota la IRA) redueix la capacitat dels asseguradors d'utilitzar el cost compartit com a eina de negociació.
La transició de l'exclusivitat de mercat és important. Després que expiri la protecció de la propietat intel·lectual, es requereix una competència robusta. Les empreses de marca tenen incentius per estendre el seu període d'exclusivitat mitjançant l'ús extensiu de patents i secrets comercials. Els fàrmacs moderns complexos sovint estan coberts per múltiples patents (sobre la molècula, el procés de producció, nous usos), cosa que pot crear un "patent thicket" que augmenta els costos d'entrada per als competidors. Mentre que algunes firmes probablement fan servir estratègies de "thicketing", el simple fet de tenir nombroses patents no prova intencions nefastes; moltes innovacions impliquen nous usos per a productes existents, que la societat pot valorar. Les preocupacions s'haurien de centrar en la validesa de les patents subjacents.
Un sistema que funcioni bé requereix una competència robusta post-exclusivitat. Per a molècules petites, els competidors genèrics poden fabricar un producte bioequivalent exacte. L'entrada de genèrics porta a grans reduccions de preus en mercats prou grans per a múltiples entrants. Tanmateix, en mercats petits, hi pot haver espai per a pocs o només un fabricant, cosa que els pot donar poder de preu. Trobar maneres de reduir els costos i retards d'entrada per als genèrics podria augmentar els beneficis per als consumidors.
Moltes innovacions recents són productes biològics de molècula gran. En aquest cas, els nous entrants creen biosimilars, que clínicament s'assemblen al producte de referència, però no són realment bioequivalents. Els mercats de biosimilars han tingut dificultats per aconseguir reduccions de preus similars a les dels genèrics. Com que no són bioequivalents, les polítiques actuals no permeten la substitució automàtica a la farmàcia. Els pacients que ja utilitzen un producte biològic de marca poden ser reticents a canviar a un biosimilar. Els fabricants de biosimilars han de comercialitzar els seus productes de manera activa.
L'estructura dels contractes de rebaixa també pot crear barreres d'entrada per als biosimilars. Els contractes per a productes incumbents poden condicionar les rebaixes a que el PBM no inclogui productes rivals (una "rebaixa mur" o "trampa"). Un patró d'aquests contractes pot desincentivar els fabricants potencials de biosimilars.
En resum, els incentius per a la innovació farmacèutica estan fortament influenciats per les barreres als nous productes i els detalls de la propietat intel·lectual. Preguntes importants inclouen la validesa de les patents addicionals, les regles per a fàrmacs de mercats petits, les regles per a l'entrada de biosimilars, i les regles que regeixen les estructures contractuals de formularis, rebaixes i cost compartit. Les empreses incumbents busquen estendre l'exclusivitat, mentre que els entrants potencials sovint estan poc representats en l'elaboració d'aquestes regles. Confiar en l'autoregulació per obtenir una regulació òptima és temerari. Aquestes qüestions reflecteixen els compromisos generals presents en un sistema que utilitza incentius de mercat per promoure i mantenir la innovació que crea benestar.

06 de juny 2025
La regulació farmacèutica als USA (3)
Lessons for the United States from Pharmaceutical Regulation Abroad
Resumit amb IA
Aquí teniu un resum detallat de l'article "Lessons for the United States from Pharmaceutical Regulation Abroad", basat en els fragments proporcionats:
L'article analitza l'economia de les regulacions farmacèutiques, centrant-se en les lliçons que els Estats Units poden aprendre d'altres països d'ingressos alts. Comença assenyalant que els preus dels medicaments als EUA, especialment els de productes amb patents, són significativament més alts que en països com França, Alemanya, Japó o el Regne Unit. Aquesta disparitat de preus alimenta el debat sobre la necessitat d'intervenció governamental als EUA.
Per què cal la intervenció governamental en els mercats farmacèutics? L'article argumenta que els mercats farmacèutics no operen sota les condicions d'un mercat competitiu ideal a causa de diverses particularitats:
- Béns de credibilitat ("Credence Goods"): És difícil per als consumidors avaluar la qualitat i els efectes dels medicaments abans i fins i tot després de consumir-los. La regulació d'entrada per part d'agències com la FDA (als EUA) o l'EMA (a Europa) busca reduir aquesta asimetria d'informació, assegurant la seguretat i l'eficàcia, però al mateix temps, significa que no hi ha lliure entrada al mercat.
- Alts costos de desenvolupament i facilitat d'imitació: El desenvolupament d'un nou fàrmac és molt car. No obstant això, un cop establerta la seva seguretat i eficàcia, la imitació és relativament fàcil. Les patents i altres formes d'exclusivitat regulatòria protegeixen els innovadors, que d'altra manera no podrien recuperar la inversió, però això és una altra raó per la qual no hi ha lliure entrada.
- Assegurança i risc moral: L'existència d'assegurances sanitàries redueix la sensibilitat dels pacients al preu real, podent portar a un consum excessiu (risc moral). Això augmenta els costos per als asseguradors. Quan els proveïdors tenen poder de mercat gràcies a les patents, poden fixar preus encara més alts.
- Prescriptors com a agents: Els metges, com a experts, medien la demanda de medicaments, però sovint no coneixen els preus relatius ni són sensibles a ells. La separació entre prescripció i dispensació, si bé ajuda a evitar problemes d'agència relacionats amb el lucre directe, limita l'elasticitat-preu dels prescriptors.
- Persistència de la informació asimètrica: Encara que la regulació redueix l'asimetria, no l'elimina. És difícil avaluar l'efecte causal d'un tractament en un individu concret. Els metges poden no estar ben informats sobre els nous desenvolupaments. La publicitat també pot influir en la demanda amb efectes ambigus. Els descomptes secrets redueixen la transparència dels preus.
Aquestes condicions creen un entorn propici per a preus molt alts en els medicaments patentats, generant desafiaments pressupostaris per als pagadors. Si els preus no reflecteixen el valor terapèutic, el mercat no envia els senyals adequats per a la direcció de la innovació. Teòricament, la intervenció governamental en la fixació de preus pot millorar els resultats.
El context dels EUA vs. altres països: Els EUA són una excepció entre els països desenvolupats per tenir un paper més limitat del govern en l'assistència sanitària i la fixació de preus de medicaments. Tot i que els preus dels medicaments són més alts, la despesa total en salut als EUA també és molt més alta. De fet, la proporció de la despesa farmacèutica dins de la despesa total en salut és la més baixa als EUA. Això suggereix que altres components de l'assistència sanitària als EUA (com els salaris de metges i infermeres) són relativament més cars.
Desafiaments de la intervenció governamental: Dissenyar un mercat centralitzat eficient és complex. La fixació de preus de medicaments és inherentment una eina de política d'innovació. Les patents, per si soles, són insuficients si els preus només busquen maximitzar el benestar estàtic; cal alinear el valor social i les recompenses privades per guiar la innovació cap a productes socialment valuosos. Mesurar el valor social d'un fàrmac és molt difícil; els assajos clínics mostren seguretat i eficàcia sota condicions controlades, no el valor terapèutic global.
Externalitats internacionals: Els medicaments són productes globalment comercialitzats. L'arbitratge de preus (comerç paral·lel/reimportació) pot fer que les empreses decideixin no llançar productes en mercats petits amb preus baixos per protegir els beneficis en països grans. Els incentius a la innovació d'un país beneficien a d'altres (efecte "spillover"). Els mercats petits tenen poc incentiu a pagar preus alts, ja que la seva contribució als ingressos globals és petita. Els mercats grans com els EUA estan subjectes al problema del "free-riding" per part d'altres països.
Tipus d'intervencions en altres països: Els governs, com a compradors monopsonistes, tenen un poder considerable. Les polítiques per controlar els preus dels medicaments patentats varien:
- Basades en costos: Regulacions de "cost-plus" o "taxa de retorn". Busquen limitar els beneficis percebuts com excessius. L'esquema del Regne Unit és un exemple de regulació de taxa de retorn a nivell de cartera. Els economistes són generalment escèptics amb aquests mètodes, especialment a nivell de producte, ja que poden recompensar la despesa en R+D ineficient i no lliguen el preu al valor terapèutic. Requereixen dades internes detallades de les empreses, que són difícils d'obtenir.
- Basades en valor: Propugnades per la indústria, on els preus es basen en el valor terapèutic (superioritat terapèutica) sense tenir en compte els costos de R+D o fabricació. Això requereix Avaluacions de Tecnologies Sanitàries (HTA) que van més enllà dels requisits d'autorització de mercat. Les HTA són costoses i consumeixen temps. La manca de coordinació entre països porta a conclusions diferents sobre el valor d'un fàrmac. Encara que s'estableixi la superioritat, queda determinar quant està disposat a pagar el pagador per aquesta millora clínica. França utilitza el SMR (servei mèdic prestat) i l'ASMR (millora del servei mèdic prestat) com a inputs per a la negociació de preus.
- Llindars de cost-efectivitat: Els pagadors utilitzen el seu poder per rebutjar la cobertura si el preu per unitat de benefici per a la salut (com un QALY - Quality-Adjusted Life Year) supera la seva disposició a pagar. El Regne Unit i Alemanya utilitzen avaluacions de cost-efectivitat com a instrument principal. Això també requereix HTA i consens sobre el valor d'una vida estadística.
Punts de referència i comerç paral·lel: Les intervencions sovint utilitzen altres preus com a referència.
- Preus de referència interns: Estableixen el nivell de reemborsament d'un nou producte igual al d'un producte competidor dins del mateix país. Permeten que els pacients paguin una prima per productes preferits, introduint certa sensibilitat al preu. L'eficiència depèn de la informació dels pacients/prescriptors i de l'elecció del producte de referència.
- Preus de referència externs: Comparen el preu del mateix producte en altres països. Molts països europeus l'utilitzen. La motivació principal sembla ser la percepció d'equitat. Un argument en contra important és que incentiva els fabricants a endarrerir el llançament (o no llançar) en els països de preus baixos que s'utilitzen com a referència, ja que el preu en aquests països afecta el preu en els països referenciadors.
- Comerç paral·lel o reimportació: Permet importar medicaments venuts a preus més baixos en altres països. Aquest arbitratge limita la capacitat de les empreses per discriminar preus entre països, la qual cosa els economistes sovint consideren relativament eficient, especialment per facilitar l'accés en països més pobres. Tant els preus de referència externs com el comerç paral·lel no han eliminat completament les diferències de preus entre països. Els preus reals reflecteixen polítiques, preferències i poder de negociació, no només el PIB per càpita.
Possibilitat d'importar polítiques als EUA: El paper més gran del sector privat i la manca de cobertura universal als EUA fan que un mateix fàrmac tingui preus molt diferents per a diferents compradors. Els PBM (Pharmacy Benefit Managers) negocien preus i col·locació al formulari, controlant l'accés a grans poblacions de pacients. A diferència dels pagadors governamentals, els PBM busquen maximitzar beneficis, no el benestar social, i poden no internalitzar els beneficis a llarg termini de la innovació. El govern federal dels EUA, tot i ser un gran pagador, va tenir un paper limitat en la negociació de preus fins recentment.
- Inflation Reduction Act (IRA) de 2022: Va introduir el Programa de Negociació de Preus de Medicaments de Medicare. Estableix un preu màxim just (MFP) per a certs fàrmacs basat en els anys des de l'aprovació, no el valor. Es temen conseqüències no desitjades, com l'endarreriment de llançaments o el "product hopping" (introduir noves versions abans que expiri la patent per evitar la negociació). Atesa la gran mida del mercat dels EUA, les seves polítiques poden afectar significativament la R+D global.
- Propostes per vincular preus als EUA amb els d'altres països: La reimportació des del Canadà s'ha proposat i fins i tot aprovat a nivell estatal per la FDA recentment. No obstant això, és probable que tingui efectes modestos en els preus globals dels EUA a causa de la petita mida del mercat canadenc, i podria reduir l'accés al Canadà. Els preus de referència externs també tenen suport bipartidista, però la indústria s'hi oposa. L'experiència europea suggereix que portaria a respostes estratègiques com l'endarreriment de llançaments i l'ús de descomptes secrets. Aquests preus no públics dificulten les avaluacions econòmiques.
En general, l'adopció de reimportació o preus de referència externs als EUA tindria efectes modestos en els preus dels EUA, però podria reduir l'accés o la transparència en altres països. La negociació de preus de Medicare (IRA) té un potencial més gran per afectar els preus als EUA i la R+D global, però el seu efecte depèn de si es basa en avaluacions de valor fiables.
Enfocaments alternatius: Davant la insatisfacció amb l'statu quo i els reptes pressupostaris que presenten teràpies molt valuoses (com Sovaldi per a l'Hepatitis C o els nous fàrmacs per a l'obesitat), s'estan considerant o experimentant alternatives:
- Contractació abans de la innovació (Ex Ante): Separar les recompenses per la innovació de les vendes amb alt marge, utilitzant pagaments fixos per a la innovació exitosa. Exemples inclouen premis o compromisos de mercat anticipats (AMCs). Els AMCs ofereixen més certesa pressupostària i clars incentius a la innovació. Exemples reals inclouen la vacuna contra el pneumococ finançada per la Fundació Gates i l'Operació Warp Speed per a les vacunes de la COVID-19. Requereixen fer moltes suposicions sota incertesa, cosa que n'explica la raresa. Pateixen del mateix risc de "free-riding" internacional.
- Contractació després de la innovació: Més fàcils d'implementar ja que mantenen el sistema de patents.
- Subhastes: S'utilitzen per a genèrics. Possible per a productes patentats si hi ha substituts propers. Les "patent buyouts" (compra de patents per part del govern per posar la propietat intel·lectual en domini públic) s'han proposat, però la seva aplicació és incerta, especialment a nivell global. Els drets de "march-in" als EUA rarament s'exerceixen.
- Preus de subscripció ("Model Netflix"): Un pagament fix al fabricant per subministrar qualsevol quantitat demandada a un preu zero o proper a zero. Proporciona certesa pressupostària i redueix l'incentiu del fabricant a comercialitzar el producte de manera inapropiada. Els desafiaments inclouen la rigidesa davant nova informació o competidors i la reducció de l'incentiu per trobar nous usos. Austràlia i alguns estats dels EUA l'han implementat per a l'Hepatitis C amb resultats mixts.
- Contractes basats en resultats ("Pay-for-performance", "Risk-sharing"): Vinculen els pagaments a la realització de fites clíniques futures. Aborden la informació imperfecta al llançament sense endarrerir l'accés i alineen els incentius del fabricant amb els resultats del pacient. No obstant això, la seva adopció es veu limitada per la dificultat de negociar-los, la manca d'evidència sobre els resultats, la infraestructura de dades insuficient i els desafiaments de mesura.
Context més ampli de la despesa sanitària: L'article conclou que, tot i l'atenció que reben els preus dels medicaments, no semblen ser el principal impulsor de l'augment total dels costos sanitaris als EUA o altres països d'ingressos alts. La competència de genèrics als EUA és generalment robusta, amb ràpida entrada i caigudes de preus després de l'expiració de patents. Els marges baixos en molts genèrics han portat a l'abandonament de fabricants i escassetats, especialment per a injectables. Els preus dels genèrics als EUA són més baixos que en països similars.
Les grans companyies farmacèutiques als EUA tenen marges de benefici i despesa en R+D significativament més alts que altres indústries. Aquesta R+D es fa amb l'expectativa de beneficis futurs. Les polítiques que redueixen els beneficis esperats disminueixen la R+D i la innovació. La mida del mercat dels EUA fa que les seves decisions polítiques siguin molt més influents en la innovació global. Les polítiques que recompensen específicament la innovació més important (com els fàrmacs orfes) semblen més exitoses. Les pròpies empreses tenen dificultats per identificar els productes més rendibles a causa del risc tècnic i de mercat, i la manca de claredat dels pagadors pot contribuir a la incertesa.
Per millorar els resultats, els responsables polítics haurien de centrar-se no només a reduir el preu mitjà o la despesa total, sinó també a acceptar preus més alts per a fàrmacs efectius, reduint les recompenses per teràpies ineficaces, i valorant els beneficis a llarg termini. Abordar les friccions i imperfeccions del mercat és crucial per augmentar l'eficiència.

Subscriure's a:
Missatges (Atom)