Detection of SARS-CoV-2 with SHERLOCK One-Pot Testing
Former posts have highlighted the potential of CRISPR for molecular diagnostics, specially in case of Covid. Now NEJM provides details of Sherlock test.

Protocol here
Detection of SARS-CoV-2 with SHERLOCK One-Pot Testing
Former posts have highlighted the potential of CRISPR for molecular diagnostics, specially in case of Covid. Now NEJM provides details of Sherlock test.
Protocol here
COVID-19 tests can be grouped as nucleic acid, serological, antigen, and ancillary tests, all of which play distinct roles in hospital, point-of-care, or large-scale population testing.Eric Topol says:
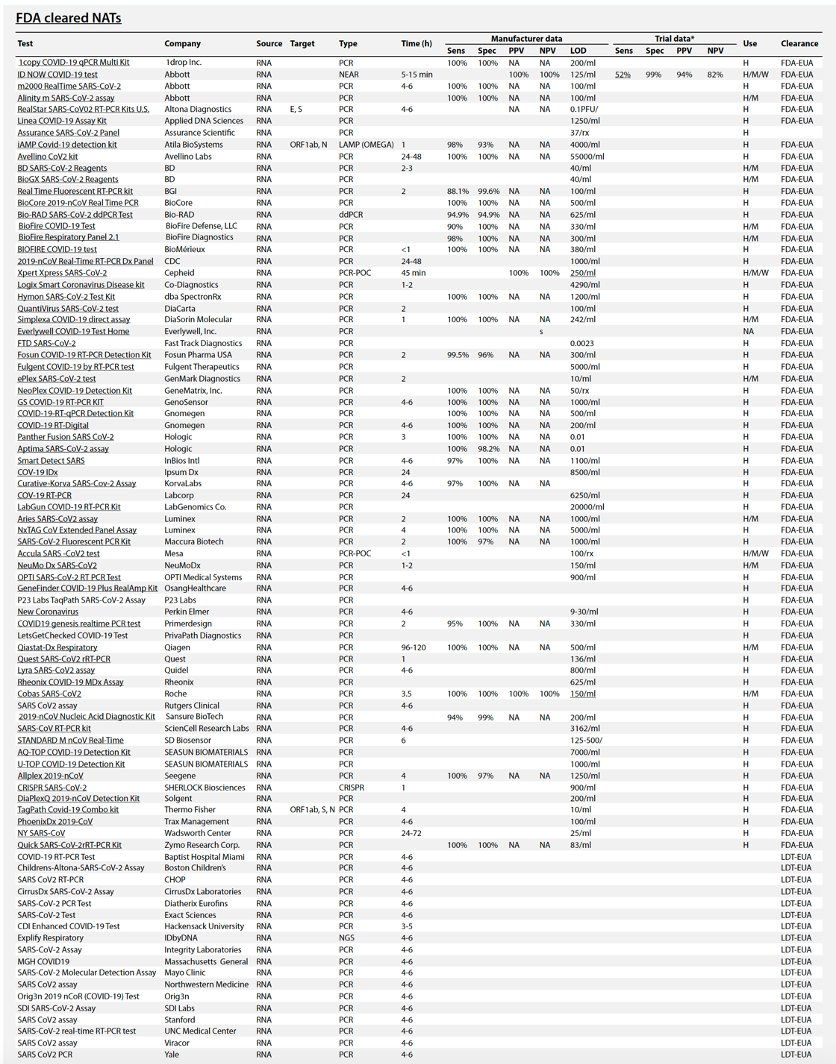
Table 1 summarizes the existing and emerging tests, current at the time of writing (May 2020). A continuously updated version of this table is available at https://csb.mgh.harvard.edu/covid
There are now *88* @US_FDA cleared (by EUA) #COVID19 tests so far. Their false negative rates range from 10-48% (by post-release reports).I agree.
Might be better to have less tests, more accuracy, with faster turnaround
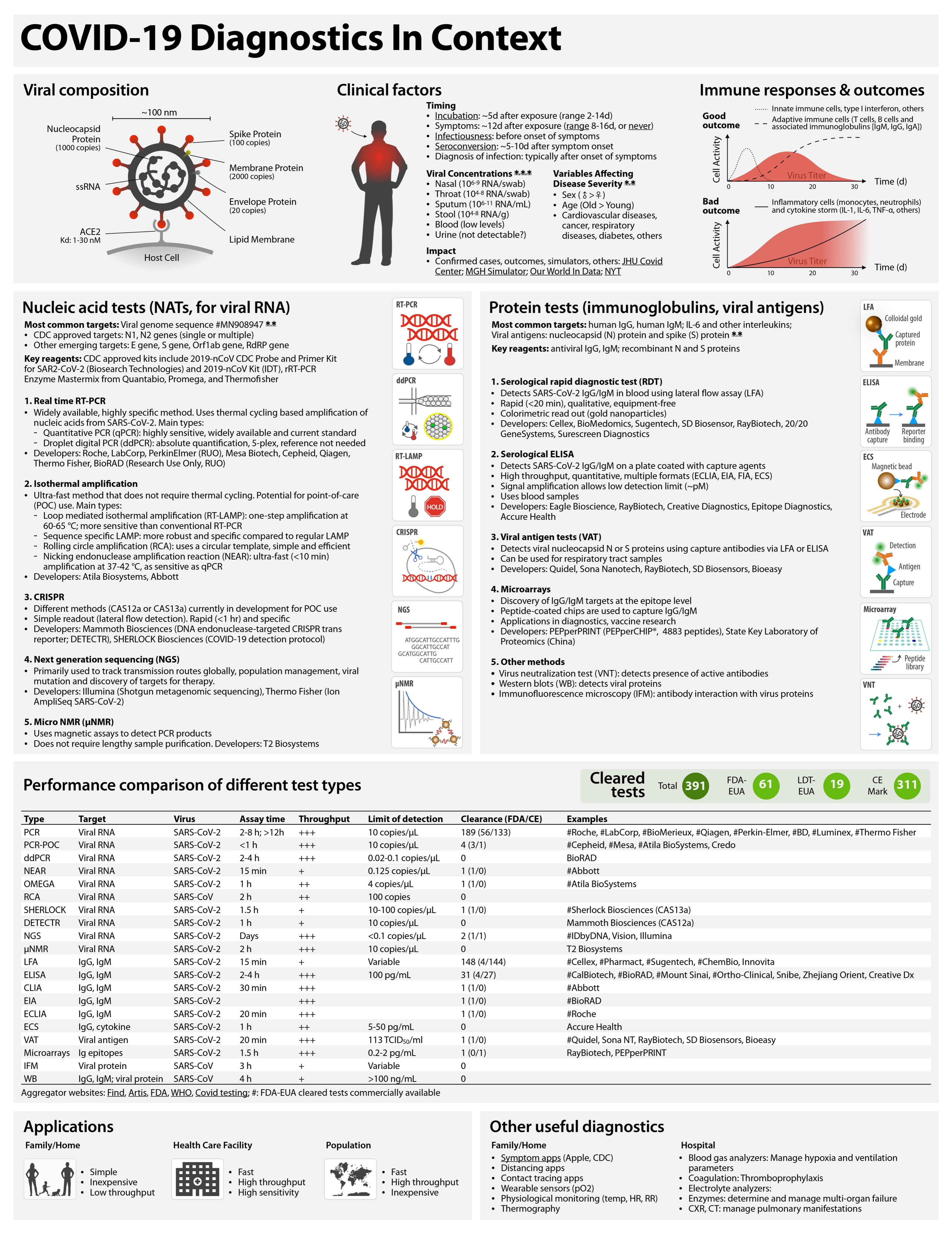
| Type | Target | Virus | Assay time | Process type | FDA-EUA | Examples |
| PCR | Viral RNA | SARS-CoV-2 | 2–8 hours; >12 hours | Plate | 56 | #Roche, #LabCorp, #BioMerieux, #Qiagen, #Perkin-Elmer, #Becton Dickinson, #Luminex, #Thermo Fisher, others |
| PCR-POC | Viral RNA | SARS-CoV-2 | <1 hour="" td=""> | Cartridge | 2 | #Cepheid, #Mesa, Credo |
| ddPCR | Viral RNA | SARS-CoV-2 | 2–4 hours | Manual | 1 | #BioRAD |
| NEAR | Viral RNA | SARS-CoV-2 | 15 min | Cartridge | 1 | #Abbott |
| OMEGA | Viral RNA | SARS-CoV-2 | 1 hour | Plate | 1 | #Atila BioSystems |
| RCA | Viral RNA | SARS-CoV | 2 hours | 0 | ||
| SHERLOCK | Viral RNA | SARS-CoV-2 | 1.5 hours | Kit | 1 | #Sherlock Biosciences (CAS13a) |
| DETECTR | Viral RNA | SARS-CoV-2 | 1 hour | Kit | 0 | Mammoth Biosciences (CAS12a) |
| NGS | Viral RNA | SARS-CoV-2 | Days | 1 | #IDbyDNA, Vision, Illumina | |
| μNMR | Viral RNA | SARS-CoV-2 | 2 hours | Cartridge | 0 | T2 Biosystems |
| LFA | IgG, IgM | SARS-CoV-2 | 15 min | Cartridge | 3 | #Cellex, #Sugentech, #ChemBio, Innovita |
| ELISA | IgG, IgM | SARS-CoV-2 | 2–4 hours | Plate | 4 | #Mount Sinai, #Ortho-Clinical (2), #EUROIMMUN US Inc., BioRAD, Snibe, Zhejiang orient, Creative Dx |
| CLIA | IgG, IgM | SARS-CoV-2 | 30 min | Cartridge | 2 | #Abbott, #DiaSorin |
| EIA | IgG, IgM | SARS-CoV-2 | 2 hours | Plate | 1 | #BioRAD |
| MIA | IgG, IgM | SARS-CoV-2 | Plate | 1 | #Wadsworth Center | |
| ECLIA | IgG, IgM | SARS-CoV-2 | 20 min | Plate | 1 | #Roche |
| ECS | IgG, cytokine | SARS-CoV-2 | 1 hour | Cartridge | 0 | Accure Health |
| VAT | Viral antigen | SARS-CoV-2 | 20 min | Cartridge | 1 | #Quidel, Sona NT, RayBiotech, SD Biosensors, Bioeasy |
| Microarrays | Ig epitopes | SARS-CoV-2 | 1.5 hours | Plate | 0 | RayBiotech, PEPperPRINT |
| IFM | Viral protein | SARS-CoV | 3 hours | Manual | 0 | |
| WB | IgG, IgM; viral protein | SARS-CoV | 4 hours | Manual | 0 |
Here we report the development and initial validation of a CRISPR–Cas12-based assay9 for detection of SARS-CoV-2 from extracted patient sample RNA, called SARS-CoV-2 DNA Endonuclease-Targeted CRISPR Trans Reporter (DETECTR). This assay performs simultaneous reverse transcription and isothermal amplification using loop-mediated amplification (RT–LAMP)14 for RNA extracted from nasopharyngeal or oropharyngeal swabs in universal transport medium (UTM), followed by Cas12 detection of predefined coronavirus sequences, after which cleavage of a reporter molecule confirms detection of the virus. We first designed primers targeting the E (envelope) and N (nucleoprotein) genes of SARS-CoV-2 (Fig. 1a). The primers amplify regions that overlap the World Health Organization (WHO) assay (E gene region) and US CDC assay (N2 region in the N gene)6,15, but are modified to meet design requirements for LAMP. We did not target the N1 and N3 regions used by the US CDC assay, as these regions lacked suitable protospacer adjacent motif sites for the Cas12 guide RNAs (gRNAs). Next, we designed Cas12 gRNAs to detect three SARS-like coronaviruses (SARS-CoV-2 (accession NC_045512), bat SARS-like coronavirus (bat-SL-CoVZC45, accession MG772933) and SARS-CoV (accession NC_004718)) in the E gene and specifically detect only SARS-CoV-2 in the N gene (Supplementary Fig. 1). This design is similar to those used by the WHO and US CDC assays, which use multiple amplicons with probes that are either specific to SARS-CoV-2 or are capable of identifying related SARS-like coronaviruses.

The FDA granted its first emergency authorization for a CRISPR-based test for COVID-19, developed by Sherlock Biosciences, designed to turn results around in about an hour compared to the four to six hours needed for other molecular diagnostics.
The test is based on the company’s namesake technology, SHERLOCK, short for Specific High-sensitivity Enzymatic Reporter unLOCKing, a Cas13a-based CRISPR system that targets RNA rather than DNA. It looks for an RNA sequence specific to SARS-CoV-2, the virus that causes COVID-19, in patient samples taken from the upper airways with a swab or from airways in the lungs known as bronchoalveolar washing.
“If it’s there, it attaches to the Cas13 enzyme and activates it, which leads to the chewing up and cleaving of RNA probes,” Sherlock CEO Rahul Dhanda told FierceMedTech. When cleaved, those RNA molecules release a fluorescent signal to show the virus is present.



We report development of a rapid (<40 accurate="" and="" as12-based="" assay="" br="" crispr="" detection="" easy-to-implement="" extracts.="" flow="" for="" from="" lateral="" min="" of="" respiratory="" rna="" sars-cov-2="" swab="">We validated our method using contrived reference samples and clinical samples from patients in the United States, including 36 patients with COVID-19 infection and 42 patients with other viral respiratory infections. Our CRISPR-based DETECTR assay provides a visual and faster alternative to the US Centers for Disease Control and Prevention SARS-CoV-2 real-time RT–PCR assay, with 95% positive predictive agreement and 100% negative predictive agreement.The role of CRISPR in diagnostics tests is going to increase.

These emerging diagnostic tools will by necessity be compared to standard diagnostics to ensure sensitivity and specificity and will need to be field-tested to guarantee performance in patient care settings, as environmental conditions and end-user application might affect performance. Proven assays, if affordable, promise to improve care in resource-limited settings where undifferentiated febrile illness is the norm and where gaps or delays in diagnosis, targeted care, and infection control contribute to infectious disease mortality and spread.More details in The Verge.
