Pharmaceutical innovation sourcing
Figure below shows that 23% of new medicines came from public bodies and private-private collaboration and they didn't apply for any marketing authorisation.

Pharmaceutical innovation sourcing
Figure below shows that 23% of new medicines came from public bodies and private-private collaboration and they didn't apply for any marketing authorisation.
A decade ago I posted this: Gestionar el declivi. John Kay said in 2011:
"When an industry model is broken, the best business strategy may be to manage its decline"
Now a new report confirms that the process continues after a decade.
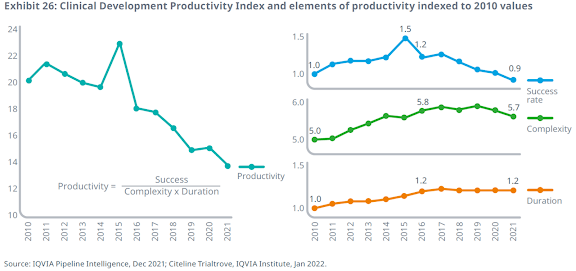
From IQVIA report:
The composite success rate across all development phases and therapy areas declined to 5.0% in 2021, which can be attributed to an appetite for increased scientific risk in clinical development programs as the bar for efficacy and safety rises, as well as increased pauses in product development due to the pandemic.
Across disease areas, probability of success varies considerably, and 2021’s composite success rate fell below the 10-year trend in all areas except for vaccines and cardiovascular.
That's all folks.
Today my suggestion is to read the post by Eric Topol with the same title.
It begins with this statement:
We’re now well over 20 years since the first human genome was sequenced, but with few exceptions the massive amount of data that has been generated has not been transformed to routine patient care.
So, why?

The Political Determinants of Health
In this book, Daniel E. Dawes argues that political determinants of health create the social drivers—including poor environmental conditions, inadequate transportation, unsafe neighborhoods, and lack of healthy food options—that affect all other dynamics of health. By understanding these determinants, their origins, and their impact on the equitable distribution of opportunities and resources, we will be better equipped to develop and implement actionable solutions to close the health gap.

Rethinking value in health innovation: from mystifications towards prescriptions
From the abstract:Debates over value in health innovation in the U.S. and Europe have
become increasingly dominated by “value-based pricing”. We examine
this prevailing narrative and its weaknesses and then present an
alternative framework for rethinking value in health. Drawing on
scholarship from the political economy of innovation, we argue that
value in health must be considered in terms of both value creation
as a collective process amongst public and private actors, as well as
value extraction that occurs due to financialization. In building this
alternative framework, we pose three questions that present areas
for further research and public policy change

The Doctor and the Algorithm. Promise, Peril, and the Future of Health AI
AI is a clear and present danger to health, safety, and equity. AI also has the potential to improve clinical care profoundly. Both of these statements are true, and both are false by dint of their incompleteness. This kind of indeterminacy is a common problem in medicine. Famously, pharmakon (the Ancient Greek word at the root of pharmacy) means “drug” but can connote either cure or poison. The Paracelsian maxim that “the dose makes the poison” is likewise a common, albeit misleading, trope of introductory pharmacology. In many ways, AI is a pharmakon. It can be both cure and poison. The indeterminacy of a pharmakon is inarguably a challenge for medicine, but it does not bring healthcare to a halt. Rather, doctors, researchers, and regulators have slowly built up, over the centuries, systems of checks and balances that ideally lead toward more pharmakon-qua-cure than pharmakon-qua-poison. Please do not misunderstand me. This has certainly not been some sort of steady progression toward a better world. I am not trying to sell a story about the inevitability of scientific progress.

The Life Worth Living. Disability, Pain, and Morality
The central argument of this book can be stated simply: the canonical idea that some lives are not worth living results from the ableist conflation of disability with pain and suffering. That is to say, the reason for this entrenched, tradition-spanning idea is the habit of thought wherein one conflates experiences of pain and suffering with experiences of disability—experiences whose form, mode, matter, or style of living is considered categorically outside ableist norms.
I offer the ableist conflation as a concept to capture the underlying presuppositions that guide ableist discourses and practices in philosophy; ethics; politics; medicine; local, national, and international policy; and beyond. Although it can take many forms, the ableist conflation involves some variation of at least the following four claims:
1. Disability necessarily involves a lack or deprivation of a natural good.
2. Deprivation of a natural good is a harm.
3. Harm causes or is itself a form of pain and suffering.6
4. Given 1–3, disability comes along with or directly causes pain and suffering.
The ableist conflation functions in part by capitalizing upon the ambiguity of the array of terms it involves. Disability, harm, pain, and suffering are all uncritically underdefined, as are the relations between them. A central goal of this book is to decouple disability and pain through phenomenological investigation and, by doing so, to dismantle the ableist conflation and the uncritical assumptions behind each of its operative terms.