Governance in healthcare institutions
As you know, in this blog I quote canadians in many respects. Their "Board of Directors Governance handbook" is a key document for those who want to understand the role of the board in a hospital. I suggest a quick look.
However, last week there was a closer presentation of a document of interest on governance by Consorci Sanitari i Social. The focus is closely related to the current trend towards converting hybrid organizations into public ones following an accounting criteria ESA-95. Some years ago I explained the big transformation in the ownership due to accounting rules! Incredible, but true.
I have always defended management autonomy and these moves were closely related towards less autonomy and more centralization. Right now, I'm repeating the same: we do need a system that is able to introduce the right governance and management. The issue is not only management autonomy it is also a responsible governance, an issue that in the past has been forgotten many times. The document shows the partial roadmap for such evolution. I would prefer to go beyond that and begin a deep review of current ownerhip and contracting in the public system, to improve efficiency.
25 de març 2014
24 de març 2014
Finding consensus in health policy
One of the key features of successful health systems is to achieve wide consensus at a societal level. Citizens have to share common values on the health system that they want. Some time ago I quoted the article by Anne Mills on this topic.
Today we can confirm that the foundations for such consensus have been built. Although unions and some parties have rejected the current text, there is a wide representation of organizations of the Catalan Council of Health. From now on, the discussion will take place in Parliament.
This is good news. You may have a look at the document here and here. There are many new insights and prescriptions to be developed.
Today we can confirm that the foundations for such consensus have been built. Although unions and some parties have rejected the current text, there is a wide representation of organizations of the Catalan Council of Health. From now on, the discussion will take place in Parliament.
This is good news. You may have a look at the document here and here. There are many new insights and prescriptions to be developed.
20 de març 2014
The seed of efficient genomic sequencing
Technology: The $1,000 genome
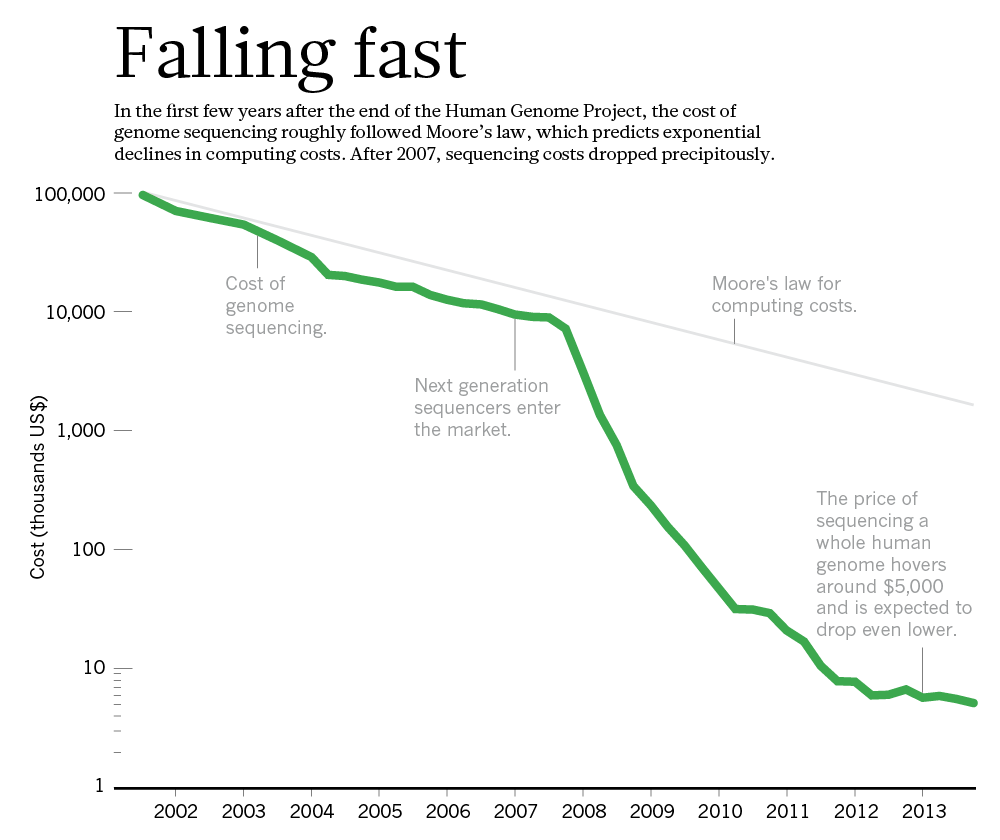
Imagine for a moment that you have back ten years, and as the health research responsible in the government you decide to allocate $230 million to achieve a $1000 individual genome sequencing. At that moment there was a monopoly by one company, Sanger. Your effort was to promote genomic applied research, better sequencing, and doing so, the monopoly would be undermined.
This is precisely what the US government did through the Advanced sequencing technology awards and right now has achieved its aim, a more efficient sequencing. They have been extremely successful and are closing the program (NHGRI) this year: the goal has been achieved.
The funds allowed to break the former monopoly (Applied Biosystems) and at the same time, ten years later, a new quasi-monopoly has appeared (Illumina). This extraordinary story is well explained in Nature:

Imagine for a moment that you have back ten years, and as the health research responsible in the government you decide to allocate $230 million to achieve a $1000 individual genome sequencing. At that moment there was a monopoly by one company, Sanger. Your effort was to promote genomic applied research, better sequencing, and doing so, the monopoly would be undermined.
This is precisely what the US government did through the Advanced sequencing technology awards and right now has achieved its aim, a more efficient sequencing. They have been extremely successful and are closing the program (NHGRI) this year: the goal has been achieved.
The funds allowed to break the former monopoly (Applied Biosystems) and at the same time, ten years later, a new quasi-monopoly has appeared (Illumina). This extraordinary story is well explained in Nature:
Researchers are optimistic that another technology will emerge to challenge Illumina. Most think, in fact, that the crucial questions for the field will shift away from technology. Now that sequencing is cheap enough to talk about scanning every patient's genome, or at least the protein-coding portion of it, it is still not clear how that information will translate into improved care (see Nature http://doi.org/rvq; 2014). These more complex issues will require another great leap in genomic science — one that could make the trouncing of Moore's law seem easy.
PS. For those that support patents, this is a good example of how prizes substitute patents to spur innovation and confirms Mckinsey article.
19 de març 2014
Medtech on the profitable road
The 2013 Medtech Value Creators Report
Finding Sustainable Value in a Changing Market
Quick numbers from US stock exchange (2009-2013) for 65 companies in Medtech sector (medical device, medical equipment, medical supply and in vitro):
Finding Sustainable Value in a Changing Market
Quick numbers from US stock exchange (2009-2013) for 65 companies in Medtech sector (medical device, medical equipment, medical supply and in vitro):
They generated a TSR (total shareholder return) of 14.8 percent per year. While in terms of value creation its performance trails that of other health-care sectors—such as health care services (at 21.5 percent per year) and biopharmaceuticals (14.9 percent per year)—it has come with less risk (that is, a smaller spread between the TSR values of the best- and the worst-performing companies), thus offering an attractive risk-reward profile for investors.That's all folks.
18 de març 2014
Futility labeling
Choosing Wisely — The Politics and Economics of Labeling Low-Value Services
As far as the evidence on effectiveness is uncertain in some cases, somebody has to put an alert on the population. Asymetric information is always moving towards some bias and favour those with better position. This is the moment for an independent body to disseminate information towards patients. In NEJM you'll find an article about Choosing wisely, an initiative already explained in this blog. An interesting objective, although the means could be controversial. Maybe professional associations are not in best position to assume such task. Kassirer (once again) reflected many years ago the relationships with industry and their conflicts of interest. My suggestion would be independent agencies, NICE style. They should inform population about what works, and they are already doing it.
As far as the evidence on effectiveness is uncertain in some cases, somebody has to put an alert on the population. Asymetric information is always moving towards some bias and favour those with better position. This is the moment for an independent body to disseminate information towards patients. In NEJM you'll find an article about Choosing wisely, an initiative already explained in this blog. An interesting objective, although the means could be controversial. Maybe professional associations are not in best position to assume such task. Kassirer (once again) reflected many years ago the relationships with industry and their conflicts of interest. My suggestion would be independent agencies, NICE style. They should inform population about what works, and they are already doing it.
16 de març 2014
Keep on improving
On the improvement of blood sample collection at clinical laboratories
Efficiency in healthcare management comes as the result of many decisions and actions. Knowledge can improve such decisions. This weekend I was reading this article on clinical labs and how to collect samples with less routes. With operations research techniques, it is possible. Afterwards there is a need to implement them. The results of the article:
Efficiency in healthcare management comes as the result of many decisions and actions. Knowledge can improve such decisions. This weekend I was reading this article on clinical labs and how to collect samples with less routes. With operations research techniques, it is possible. Afterwards there is a need to implement them. The results of the article:
The two laboratories in this study previously planned routes manually for 43 and 74 collection points, respectively. These routes were covered by an external carrier company. With the implementation of this algorithm, the number of routes could be reduced from ten to seven in one laboratory and from twelve to nine in the other, which represents significant annual savings in transportation costsThe potential for operations research in healthcare is huge. The incentives to apply it, low (unfortunately).
13 de març 2014
Commercialism in health and medicine
Buying Health: The Costs of Commercialism and an Alternative Philosophy
There are only three topics of health policy in the newspapers (unfortunately): waiting lists, copayments and privatization. As soon as one topic drops from the agenda, the informational cascade starts with the following one. The last one, privatization is still a concept in need of definition and measurement. I already covered this issue last year and I don't want to repeat it.
Today I would like to insist that beyond a new framing of the concept, maybe we have to change the scope and the term. The right term could be commercialism. We have to understand better how and when commercialism is undermining professionalism.
Jerome Kassirer wrote an excellent piece (US oriented) in Cambridge Quarterly of Healthcare Ethics some years ago that it is still a reference for today. His words:
Churchill and Churchill go beyond the usual scope. Their recent article abstract says:
There are only three topics of health policy in the newspapers (unfortunately): waiting lists, copayments and privatization. As soon as one topic drops from the agenda, the informational cascade starts with the following one. The last one, privatization is still a concept in need of definition and measurement. I already covered this issue last year and I don't want to repeat it.
Today I would like to insist that beyond a new framing of the concept, maybe we have to change the scope and the term. The right term could be commercialism. We have to understand better how and when commercialism is undermining professionalism.
Jerome Kassirer wrote an excellent piece (US oriented) in Cambridge Quarterly of Healthcare Ethics some years ago that it is still a reference for today. His words:
Professionalism is fundamentally a pact with society. In recognition of certain behaviors and attributes, society confers professional status on us. These privileges are not bestowed, but are earned, and they must be renewed repeatedly for the status to be preserved. Professional behaviors include technical competence that is valued and that adds value, a commitment to self-improvement, a commitment to selfmonitoring and self regulation, and a commitment to use the unique knowledge and competence for the best interests of our patients. This last requirement should include a commitment to resolve conflicts of interest in our patients’ favor.
Is money trumping professionalism? Certainly the pharmaceutical money tsunami is having major adverse effects. It tends to distract faculty into emphasizing profitable research and to neglect their teaching duties. It replaces openness with secrecy, it privatizes knowledge, and it replaces part of the social commons by commercializing discovery. In many instances, it downplays knowledge as a social good. It has also created a culture within which the design of studies is sometimes jiggered to create positive results, in which unfavorable results are sometimes buried, where communication of results is sometimes hindered for commercial reasons, and where bias in publications and educational materials has gone completely uncheckedMaybe there are excessive generalizations, but take it as a general statement to be confirmed by facts and data.
Churchill and Churchill go beyond the usual scope. Their recent article abstract says:
This paper argues that commercial forces have steadily encroached into our understanding of medicine and health in modern industrial societies. The impact on the delivery of personal medical services and on common ideas about food and nutrition is profound and largely deleterious to public health. A key component of commercialization is reductionism of medical services, health products and nutritional components into small, marketable units. This reductive force makes both medical services and nutritional components more costly and is corrosive to more holistic concepts of health. We compare commercial and holistic approaches to nutrition in detail and offer an alternative philosophy. Adopting this alternative will require sound public policies that rely less on marketing as a distribution system and that enfranchise individuals to be reflective on their use of medical services, their food and nutrition choices, and their larger health needsI deeply agree with such perspective.
12 de març 2014
Against patents, again
Deadly Monopolies: The Shocking Corporate Takeover Of Life Itself – And The Consequences For Your Health And Our Medical Future
I've just finished reading a book on patents in life sciences. As you know from previous posts , I'm convinced that there is an enormous welfare loss from current patent system. If you have the opportunity to read this book, you'll finally will arrive at the same conclusion. Although it was written before the Supreme Court ruling over the Myriad case, the message is still the same: patents contrain innovation and are extremely costly to the society. The case of Hepatitis C is explained in detail. Until some patents were exhausted there was no possibility to start research. Without such patents, new succesful and (costly) treatments have arisen (and afterwards have been patented again).
An interesting interview in Forbes magazine highlights the key issues of the book. Unfortunately times go by and alternatives to patents are not taking off.
I've just finished reading a book on patents in life sciences. As you know from previous posts , I'm convinced that there is an enormous welfare loss from current patent system. If you have the opportunity to read this book, you'll finally will arrive at the same conclusion. Although it was written before the Supreme Court ruling over the Myriad case, the message is still the same: patents contrain innovation and are extremely costly to the society. The case of Hepatitis C is explained in detail. Until some patents were exhausted there was no possibility to start research. Without such patents, new succesful and (costly) treatments have arisen (and afterwards have been patented again).
An interesting interview in Forbes magazine highlights the key issues of the book. Unfortunately times go by and alternatives to patents are not taking off.
10 de març 2014
Health impact of sugar-sweetened beverages taxation
Averting Obesity and Type 2 Diabetes in India through Sugar-Sweetened Beverage Taxation: An Economic-Epidemiologic Modeling Study
Clever politicians want to know the potential welfare impact of taxation. I said "clever", though this is not always the case. An example of economic modeling for sugar-sweetened beverages to set up the right level of taxation (in India), appears in PLOS Medicine. The summary:
The documentary is about weight control, but places special emphasis on sugar (addiction). Please have a look at the quantity of sugar in a beverage!!! (14 sugar cubes). Incredible.
PS. "Superbe" post by Reinhardt: How the Medical Establishment Got the Treasury’s Keys
Clever politicians want to know the potential welfare impact of taxation. I said "clever", though this is not always the case. An example of economic modeling for sugar-sweetened beverages to set up the right level of taxation (in India), appears in PLOS Medicine. The summary:
The researchers used survey data relating SSB consumption to price variations to calculate how changes in the price of SSBs affect the demand for SSBs (own-price elasticity) and for other beverages (cross-price elasticity) in India. They combined these elasticities and data on SSB sales trends, BMIs, and diabetes incidence (the frequency of new diabetes cases) into a mathematical microsimulation model to estimate the effect of a 20% tax on SSBs on caloric (energy) consumption, glycemic load (an estimate of how much a food or drink raises blood sugar levels after consumption; low glycemic load diets lower diabetes risk), the prevalence of overweight/obesity, and the incidence of diabetes among Indian subpopulations. According to the model, if SSB sales continue to increase at the current rate, compared to no tax, a 20% SSB tax would reduce overweight/obesity across India by 3.0% and the incidence of type 2 diabetes by 1.6% over the period 2014–2023. In absolute figures, a 20% SSB tax would avert 11.2 million cases of overweight/obesity and 400,000 cases of type 2 diabetes between 2014 and 2023. Notably, if SSB sales increase more steeply as predicted by drinks industry marketing models, the tax would avert 15.8 million cases of overweight/obesity and 600,000 cases of diabetes. Finally, the model predicted that the largest relative effect of an SSB tax would be among young men in rural areas.The results confirm previous studies, 20% may be the ceiling for a tax . But what happens to health?. Assumptions on a fall in consumption, are just that, assumptions. And former behaviour is extrapolated into the future. This is what happens to any model, and this is the uncertainty and courage that any politician must hold in taking a difficult decision. Such moment is closer than before. If you are not convinced, I would suggest you have a look at this documentary released last week:
The documentary is about weight control, but places special emphasis on sugar (addiction). Please have a look at the quantity of sugar in a beverage!!! (14 sugar cubes). Incredible.
PS. "Superbe" post by Reinhardt: How the Medical Establishment Got the Treasury’s Keys
07 de març 2014
Cost-effectiveness with uncertain effectiveness
Gene expression testing is quite different from genetic testing. Gene expression refers to epigenetic regulation of genes that occur without alteration of DNA. I've covered such topics several times in this blog. Today, I would like to focus on a recent published work on a new test that assesses whether or not a patient's chest discomfort or other symptoms are due to obstructive coronary artery disease. Sounds interesting, since angiography is a costly technology.
A quick look at this recent article will raise new doubts. As you know, there is no need for cost-effectiveness analysis when effectiveness is uncertain. When talking about testing effectiveness means, sensitivity and specificity, AUC and so on. But what happens when the seller (or the model) decides about the threshold and afterwards focuses on negative predictive value of 96% and provides the desired value?. The threshold is only an option in the model. Why not change it?. There is a circular reasoning on that.
My concern is that health economics should look in detail at such issues. It is not an issue of conflicts of interest. In this case any health economist should avoid entering such territory.
05 de març 2014
When asking your physician is not enough
23andMe and the FDA
Some weeks ago I explained the FDA "closure" of DTC genetic testing business. NEJM analyses with detail the rationale behind such policy:
Some weeks ago I explained the FDA "closure" of DTC genetic testing business. NEJM analyses with detail the rationale behind such policy:
The goal of the FDA and 23andMe (as well as all clinical geneticists, testing laboratories, and the entire genetics industry) should be to ensure that genomic information is both accurate and clinically useful. Clinicians will be central to helping consumer–patients use genomic information to make health decisions. Any regulatory regime must recognize this reality by doing more than simply adding the tagline on most consumer ads for prescription drugs: “Ask your physician.” That is insufficient guidance unless your physician has ready access to a clinical geneticist or genetic counselor.European regulation is 15 years old and the new directive is still being discussed. It will not be applied for at least 3 years. Meanwhile, do you know who is protecting us from inaccurate and clinically useless information?
04 de març 2014
Let's get fit, not fat
Aportaciones de la economía del comportamiento en política sanitaria: Algunas notas en torno al ejemplo de la obesidad
The influence of obesity and overweight on medical costs: a panel data perspective
In the EJHE you'll find a clear message:
The EEA article by A. Garcia-Altés reflects current knowledge on behavioral economics and obesity. However there is a long way to go. As I said in a former post we do need a battery of measures to fight obesity: regulatory, social and individual measures.
The influence of obesity and overweight on medical costs: a panel data perspective
In the EJHE you'll find a clear message:
The results indicate that obesity is associated with substantial healthcare cost increases and there are large differences in costs by degree of obesity. Specifically, severe obesity raises total direct medical costs by an average of 160 € per patient and year. With total medical costs averaging 600 € for normal-weight individuals, this means that severe obesity is associated with an increase in costs of 26 %. The effect of moderate obesity is more modest: it raises medical costs by 97 € or 16 %. Overweight has an even smaller impact, raising costs by 51 € or 8.5 %.Therefore, if obesity has an economic and health impact, what next?
The EEA article by A. Garcia-Altés reflects current knowledge on behavioral economics and obesity. However there is a long way to go. As I said in a former post we do need a battery of measures to fight obesity: regulatory, social and individual measures.
28 de febrer 2014
Our irrational behaviour
The Behavioral Economics of Health and Health Care
Irrationality in Health Care: What Behavioral Economics Reveals About What We Do and Why
Thomas Rice provides an overview of behavioral economics in health in a recent article in Annual review of public health. More or less the same things we already know with some concrete messages. A good starting point for those that want to take first steps in this discipline. The summary:
Thomas Rice says in this respect:
PS. For those interested in an introductory course, on March 11th starts at Coursera: A Beginner's Guide to Irrational Behavior
Irrationality in Health Care: What Behavioral Economics Reveals About What We Do and Why
Thomas Rice provides an overview of behavioral economics in health in a recent article in Annual review of public health. More or less the same things we already know with some concrete messages. A good starting point for those that want to take first steps in this discipline. The summary:
People often make decisions in health care that are not in their best interest, ranging from failing to enroll in health insurance to which they are entitled, to engaging in extremely harmful behaviors. Traditional economic theory provides a limited tool kit for improving behavior because it assumes that people make decisions in a rational way, have the mental capacity to deal with huge amounts of information and choice, and have tastes endemic to them and not open to manipulation. Melding economics with psychology, behavioral economics acknowledges that people often do not act rationally in the economic sense. It therefore offers a potentially richer set of tools than provided by traditional economic theory to understand and influence behaviorsRight now behavioral economics is still a promise, let's wait until we can really apply it widely.
Thomas Rice says in this respect:
With the exception of Kahneman & Tversky’s prospect theory, which was developed more than 30 years ago, there has been little in the way of bringing the various tools and policies of behavioral economics under one umbrella. As a result, most of the applications seem to be ad hoc. More development of an overarching theory could aid those interested in designing new interventions when it is clear that traditional economics remedies are insufficientRegarding the book on Irrationality in Health Care, I haven't had the opportunity to have a look at it. I leave here the reference and 23 anomalies . Maybe in the book there is the answer to solve them.
PS. For those interested in an introductory course, on March 11th starts at Coursera: A Beginner's Guide to Irrational Behavior
27 de febrer 2014
Hostis populi
A plot written by Ibsen in 1882 could reflect current conflicts nowadays. Whats first: Your money or your health?. I went to the theatre last week. Great "mise en escène".
The summary:
The summary:
Doctor Thomas Stockmann is a popular citizen of a small coastal town in Norway. The town has invested a large amount of public and private money towards the development of baths, a project led by Stockmann and his brother, Peter, the Mayor. The town is expecting a surge in tourism and prosperity from the new baths, which are said to be of great medicinal value, and as such, a source of great local pride. Just as the baths are proving successful, Stockmann discovers that waste products from the town's tannery are contaminating the waters, causing serious illness amongst the tourists. He expects this important discovery to be his greatest achievement, and promptly sends a detailed report to the Mayor, which includes a proposed solution which would come at a considerable cost to the town.I deeply disagree with this final generalization. The details are important.
To his surprise, Stockmann finds it difficult to get through to the authorities. They seem unable to appreciate the seriousness of the issue and unwilling to publicly acknowledge and address the problem because it could mean financial ruin for the town. As the conflict develops, the Mayor warns his brother that he should "acquiesce in subordinating himself to the community." Stockmann refuses to accept this, and holds a town meeting at Captain Horster's house in order to persuade people that the baths must be closed.
The townspeople — eagerly anticipating the prosperity that the baths will bring — refuse to accept Stockmann's claims, and his friends and allies, who had explicitly given support for his campaign, turn against him en masse. He is taunted and denounced as a lunatic, an "Enemy of the People." In a scathing rebuttal of both the Victorian notion of community and the principles of democracy, Stockmann proclaims that, in matters of right and wrong, the individual is superior to the multitude, which is easily led by self-advancing demagogues. Stockmann sums up Ibsen's denunciation of the masses with the memorable quote "...the strongest man in the world is the man who stands most alone." He also says: "A minority may be right; a majority is always wrong.
Subscriure's a:
Missatges (Atom)