From NRD

From Nature NRD


Because pathology and radiology have a similar past and a common destiny,
perhaps these specialties should be mergedinto a single entity, the “information specialist,” whose responsibility will not be so much to extract information from images and histology but to manage the information extracted by artificial intelligence in the clinical context of the patient.
There may be resistance to merging 2 distinct medical specialties, each of which has unique pedagogy, tradition, accreditation,and reimbursement.However, artificial intelligence will change these diagnostic fields. The merger is a natural fusion of human talent and artificial intelligence. United, radiologists and pathologists can thrive with the rise of artificial intelligence.
The history of automation in the broader economy has a reassuring message. Jobs are not lost; rather, roles are redefined; humans are displaced to tasks needing a human element. Radiologists and pathologists need not fear artificial intelligence but rather must adapt incrementally to artificial intelligence, retaining their own services for cognitively challenging tasks.A unified discipline, information specialists would best be able to captain artificial intelligence and guide medical information to improve patient care.You may agree or not. Technology is breaking barriers and creating bridges. Food for thought.

"As machines get smarter, humans will need to evolve along a different path from machines and become more humane"This may be Eric Topol's desire, nothing to add. My view is quite different. I'm not sure about the contribution of AI to a humanised medicine . This has to do with professionalism, not with AI. And the incentives for professionalism are plunging, while commercialism is on the rise. This is the key issue.

An advisory panel to the World Health Organization has called for the creation of a global registry to monitor gene-editing research in humans, the organization announced yesterday (March 19). The recommendations of the 18-person committee, which was established following news late last year that Chinese scientist He Jiankui had carried out human gene editing in secret, are aimed at improving transparency and responsibility in the field, the announcement says.
The panel’s advice did not go so far as to call for a moratorium on all human germline editing, unlike some other groups. Last week, a group of scientists and bioethicists from seven countries penned a commentary in Nature that argued for “a fixed period during which no clinical uses of germline editing whatsoever are allowed.” Such a moratorium would allow time for ethical and moral debate and for the agreement of an international regulatory framework, they wrote.After the initial #CRISPRbabies scandal , we are facing a new one. The WHO pannel is asking for a registry instead of a moratorium. The battle has finished. Game over. From now on, the human being will be affected from such decision. One of the worst decisions in the human history.

This report provides an overview of patient-level data on medicines routinely collected in health systems from administrative sources, e.g. pharmacy records, electronic health records and insurance claims. In total 26 OECD and EU member countries responded to a survey addressing the availability and accessibility of routinely collected data on medicines and their applicability to developing evidence. The report further explores the utility of evidence from clinical practice, looking at experiences and initiatives across the OECD and EU.Governments will have to improve big data capabilities and add new talent.

Our findings offer perhaps the strongest evidence to date that insurance reveal as much or more about consumer understanding than about actual health-related risk preferences. In this sense, our setting provides a rare opportunity to conduct a specification check on
the standard insurance demand model absent search frictions.
Our findings challenge the standard practice of inferring risk preferences from insurance choices and raise doubts about the welfare benefits of health reforms that expand consumer choice.If this is so, many books should be rewritten asap.
1. A country spends 38m € in drugs for 249 patients in 2018. A lifetime treatment.
2. A country has a waiting list of 132.025 patients for surgery, 123.249 patients for diagnostic tests, and 424.715 patients waiting for a visit to the specialist. Total people waiting: 679.989 patients in a country with 7.543.825 inhabitants. 9% of the population is in the waiting list for a health service. However, 25% have voluntary duplicate insurance and could jump the list. Therefore the exact figure is 12% of inhabitants waiting.
3. A country knows that spending 10m € in addition every year can increase cardiac surgery by 600 interventions. This means 600 critical patients less in the waiting list. With 38m €, the number of cardiac interventions would be 2.280.Ask yourself what to do about it, what would you prefer to do with 38m€ every year ? Just apply them to 249 patients or to 2.280 (you are not on the waiting list, and we'll assume the same adjusted quality of life years for both cases). Anyway, it's too late to have your answer, the government has already decided for you, and maybe you don't agree with it, as I don't agree. The government prefers the rescue of 249 citizens.
This country spends 1.192 € per capita of public budget on health. Another country under the same mandatory tax system is able to spend 1.635 €, 40% more !!!More money allows to avoid such dilemmas for this country. Ask yourself if you want to stay in the former tax system that is damaging your health. Once you have the answer, you'll understand why this country wants to leave this unfair tax system as soon as possible.

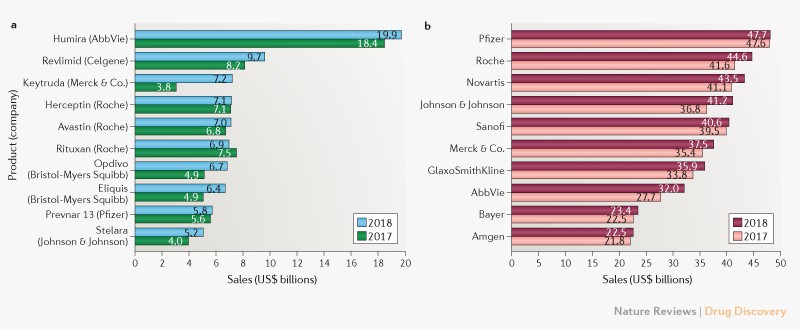
The growing cost of new drugs includes buying companies for their research (outsourcing research) instead of "producing" R&D within the company. The report will not tell you this minor observation.
- R&D returns have declined to 1.9 per cent, down from 10.1 per cent in 2010 - the lowest level in nine years
- Returns have been impacted by the growing cost of bringing a drug to market which now stands at $2,168 million – almost double the $1,188 million recorded in 2010
- Forecast peak sales have declined from last year to $407 million – less than half the 2010 value of $816 million
In drug industry the probability of R&D failure is 90.4%. We all know that in the drug costs we are paying also for failures, but we easily forget the figure.You'll not find any reference to this minor issue. Is there any profitable industry with such a failure rate?
The use of AI raises ethical issues, including:This statement is naive.(From m-w, naive: marked by unaffected simplicity : INGENUOUS). Up to now, have you seen any transparent algorithm available for imaging, triage or any medical app? For sure not. Therefore, the real key challenge is to stop introducing such algorithms -to ban apps- unless there is a regulatory body that takes into account the quality assurance or effectiveness side (sensitivity and specificity) and the required transparency for citizens.
- the potential for AI to make erroneous decisions;
- the question of who is responsible when AI is used to support decision-making;
- difficulties in validating the outputs of AI systems; inherent biases in the data used to train AI systems;
- ensuring the protection of potentially sensitive data;
- securing public trust in the development and use of AI;
- effects on people’s sense of dignity and social isolation in care situations;
- effects on the roles and skill-requirements of healthcare professionals;
A key challenge will be ensuring that AI is developed and used in a way that is transparent and compatible with the public interest, whilst stimulating and driving innovation in the sector.
- and the potential for AI to be used for malicious purposes.
To unlock the potential of advanced analytics while protecting patient safety, regulatory and professional bodies should ensure that advanced algorithms meet accepted standards of clinical benefit, just as they do for clinical therapeutics and predictive biomarkers. External validation and prospective testing of advanced algorithms are clearly neededThey explain the five standards and give rules and criteria for regulation. It is really welcome.

Precision medicines inherently fragment treatment populations, generating small-population markets, creating high-priced “niche busters” rather than broadly prescribed “blockbusters”. It is plausible to expect that small markets will attract limited entry in which a small number of interdependent differentiated product oligopolists will compete, each possessing market power.A chapter in a new book on Precision Medicine explains the new approaches to a oligopolistic market structure where the size of the market may be determined by biomarkers with a cut-off value suggested by pharmaceutical firms themselves. The dynamics of this market is described according to game theory. Sounds fishy at least.