It is perhaps more useful to imagine an algorithm as existing along a
continuum between fully human-guided vs fully machine-guided data
analysis. To understand the degree to which a predictive or diagnostic
algorithm can said to be an instance of machine learning requires
understanding how much of its structure or parameters were predetermined
by humans. The trade-off between human specification of a predictive
algorithm’s properties vs learning those properties from data is what is
known as the machine learning spectrum
Higher placement on the machine learning spectrum does not imply
superiority, because different tasks require different levels of human
involvement. While algorithms high on the spectrum are often very
flexible and can learn many tasks, they are often uninterpretable and
function mostly as “black boxes.” In contrast, algorithms lower on the
spectrum often produce outputs that are easier for humans to understand
and interpret.
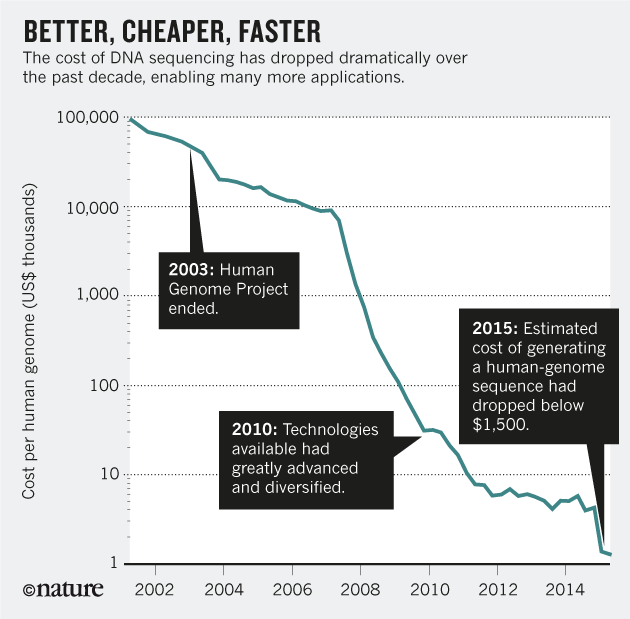
Where does DNA sequencing goes from here?. Nowadays, this is an appropriate question to pose. The answer appears in an article in an interesting article in Nature.
Now, geneticists would like to have DNA sequences for everyone on Earth, and from every cell in every tissue at every developmental stage (including epigenetic modifications), in health and in disease. They would also like to get comprehensive gene-expression patterns by sequencing the complementary DNA copies of messenger RNA molecules.
In a mere 40 years, the central goal of putting molecular data about cells to practical use has changed from an informational challenge to a meta-informational one. Take clinical applications of genome-sequence data. It may soon be possible to use DNA sequencing routinely to analyse body fluids obtained for any clinical purpose. But only a vast amount of well-organized data about the multi-year medical histories of millions of people will provide the meta-information needed to establish when to ignore such data and when to act on them.
A research on seven top pharmaceutical companies has provided fresh data about costs of clinical trials:
For the trials in the data set, the median cost of conducting a study from protocol approval to final clinical trial report was US$3.4 million for phase I trials involving patients, $8.6 million for phase II trials and $21.4 million for phase III trials.
If you compare these data with the total drug costs (2.6 billion), you may ask yourself how all these costs are estimated. Maybe all this information is wrong and useless.
If you want to know an updated approach to policy reforms, then you have to read the World Development Report 2017
The main messages:
Successful reforms are not just about “best practice.” To be effective, policies must guarantee credible commitment, support coordination, and promote cooperation.
Power asymmetries can undermine policy effectiveness. The unequal distribution of power in the policy arena can lead to exclusion, capture, and clientelism.
Change is possible. Elites, citizens, and international actors can promote change by shifting incentives, reshaping preferences and beliefs, and enhancing the contestability of the decision making process.
Three guiding principles for rethinking governance for development are:
Think not only about the form of institutions, but also about their functions.
Think not only about capacity building, but also about power asymmetries.
Think not only about the rule of law, but also about the role of law
You'll understand that the key element of any reform goes beyond evidence on what works and consensus. It should be clearly designed following specific steps. I suggest you have a look at it.
I've said it many times: beware of snake-oil sellers. Nowadays you may find it everywhere, specially on internet. You may get a genetic test for a disease that creates a false illusion of safety, or another that provides an unnecessary and avoidable concern. Only evidence based prescribed tests can be considered appropriate.
Therefore, if you want to confirm that genome is not enough, you have to check the review at NEJM on epigenetics. At the end of the article you'll find the explanation on why we do need integrated genome and epigenome association studies. You'll understand that cancer is fundamentally an epigenetic disease.
The current knowledge is changing quickly some conventional truths and "known unknowns" that we've had for years. This is good news for citizens, and bad news for snake-oil sellers if detected. Governments should help citizens on this screening effort, and protect citizens from fake medical information.
Why is it so difficult to accept it? There is wide "evidence for the practice-makes-perfect hypothesis by showing that volume is a driving factor for quality". Unfortunately, the opportunities for the health system are still larger than it should be. There is a resistance in organizations, there is inertia, and all these drivers play a role. In planned health systems, there is no reason to be strict on it.
Just for those that are dubious, I would suggest a look at this article and to my former post.
It's about Theranos. You may find my previous posts in this link. Now SEC has confirmed that was a "massive fraud". That's it. If you want a good analysis check FT.
Microfluidics is not an easy prêt-à-porter technology. Many people knew it but Mrs Holmes has been selling it as snake-oil. And as usual in these cases, the end of the film is already written. She can't go to the lab for the next 10 years, a fine, and the company may be closed. All started with and article by Mathew Herper in WSJ. An innocent article with an innocent question that she couldn't answer. That's all. Silicon valley smart money would not have made this mistake.