The COVID-19 Pandemic and the $16 Trillion Virus
Summary of the estimates by Cutler and Summers:

And a video:
The COVID-19 Pandemic and the $16 Trillion Virus
Summary of the estimates by Cutler and Summers:
And a video:
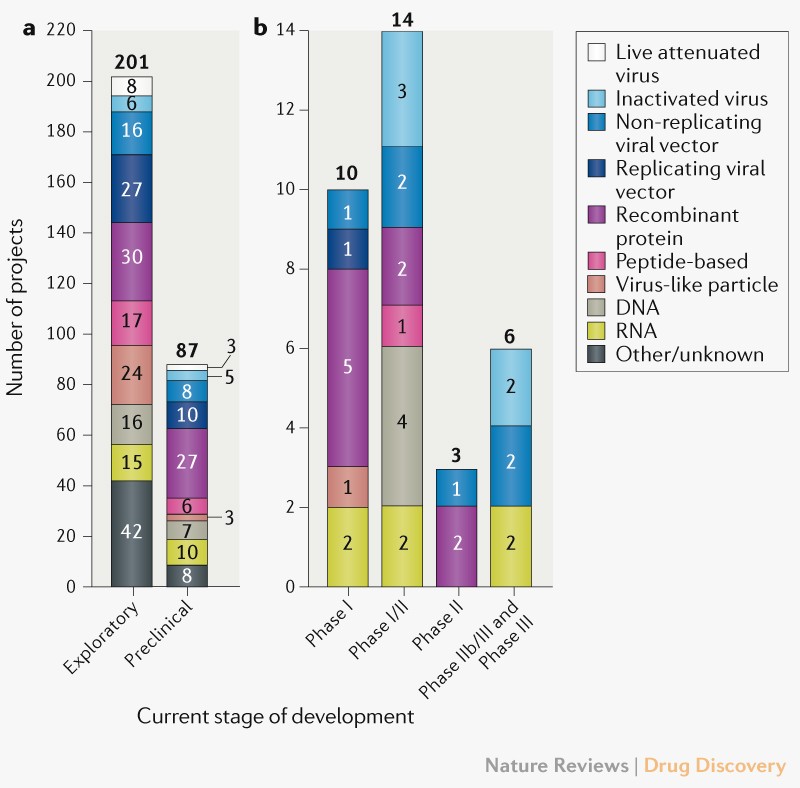
Evolution of the COVID-19 vaccine development landscape
Currently there are 321 vaccine candidates for COVID, however only 33 have entered clinical trials.
Although the leading COVID-19 vaccine candidates have progressed to advanced stages of clinical development at exceptional speed, many uncertainties remain given the lack of robust clinical data so far. Moreover, given the highly unusual circumstances associated with developing a vaccine during the evolution of a novel global pandemic, probability of success benchmarks for traditional vaccine development are likely to underrepresent the risks associated with delivering a licensed vaccine for COVID-19. The most advanced candidates are expected to begin reporting data from pivotal studies over the coming months, which if positive will be used to support accelerated licensure of the first COVID-19 vaccines.
Norbert Goldfield et al provides a useful reflection on the current moment in US. And says:
The virus has exposed glaring weaknesses that cannot be unseen. The US health care system’s embrace of patient-centered care is being tested.
We need a new paradigm, one that moves from a patient-centered care system to a community-centered health and social care ecosystem. Unlike much of the current US medical care system, the community sector has lacked funding and development. Strong and consistent sources of support are needed to make this sector viable and keep it flourishing.
Politics will ultimately determine how our current patient-centered acute care–focused health care system will change. The wealthy undoubtedly will continue to have an outsize influence on any legislation promoting CCPH. Despite this fact, we will at least think about becoming better in improving our response before the next pandemic hits.
Both articles deserve being read.

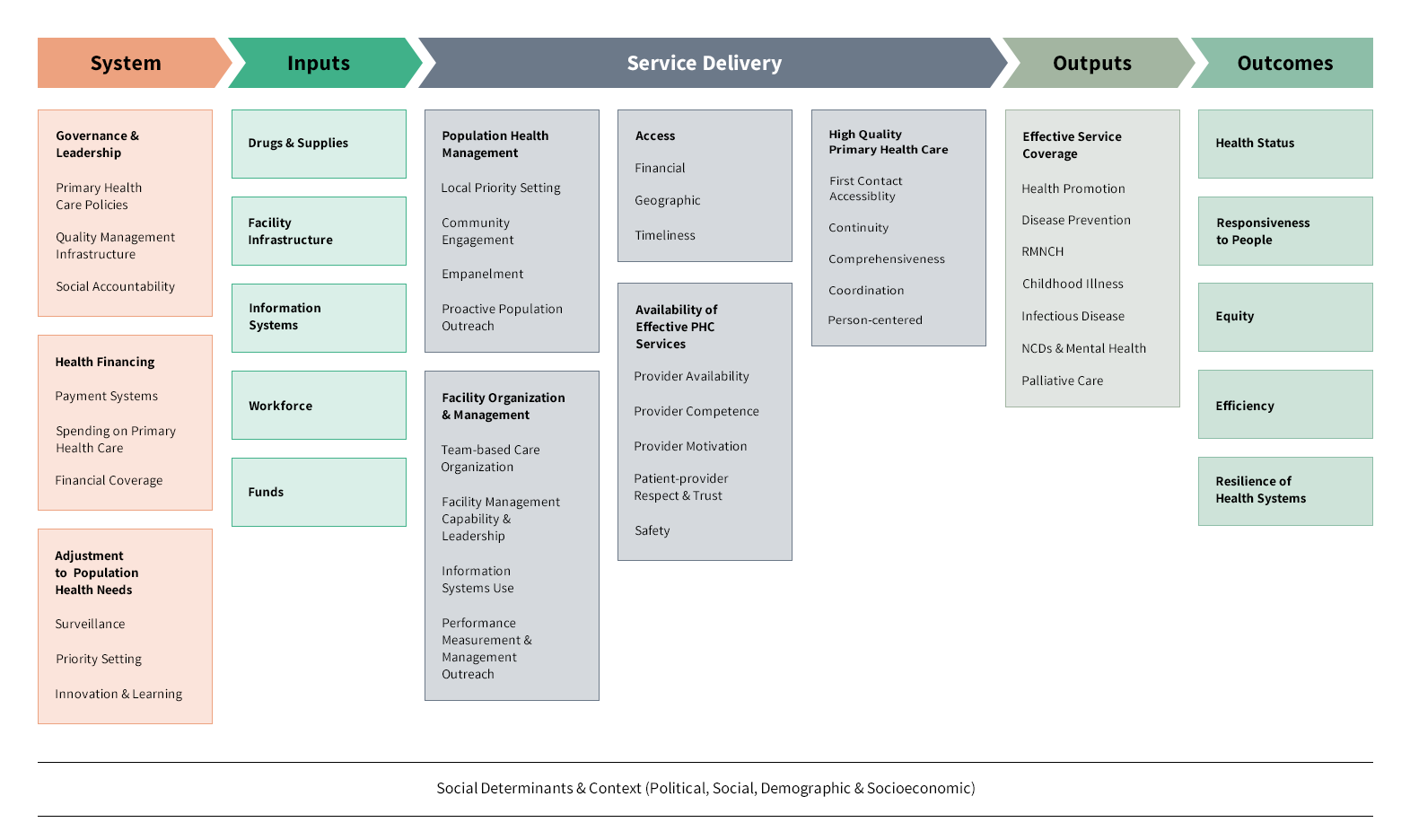
Taking Stock of the Global Primary Health Care Measurement Landscape
During the pandemic everybody agree about the need for a strong primary care. What does this mean?
Check this framework:
Dual practice refers to physicians concurrent activity, public and private. The conflicts of incentives arise and some regulatory mechanisms are needed.
The regulatory mechanisms that have been employed across countries can be divided into three categories: those that advocate for total banning of DP, those that allow it with restrictions and those that allow it without restriction. Countries that attempted total banning of dual practice, as in Portugal and Greece, could not easily stamp it out. DP continued to exist on a wide scale in Portugal until the ban was lifted in 1993 (Oliveira and Pinto, 2005). Similarly, the ban in Greece from 1983 to 2002 did not prevent public doctors from practising privately (Mossialos et al., 2005). Efforts to ban dual practice failed because of lack of capacity to enforce it. The resources needed to enforce it may not be commensurate with the benefits a country gets from banning it. Moreover, banning dual practice has in some countries been associated with the migration of health workers, especially specialists, from the public to the private sector as well as an international brain drain (Buchan and Sochalski, 2004; Mossialos et al., 2005). In LMIC settings where health workers are underpaid and members of the general population are willing to pay for more convenient and possibly better services, this option might not be viewed as legitimate or even feasible.
The second category is allowing dual practice with restrictions. This was the most frequent approach used by countries. Financial and licensure restrictions as well as promotional incentives were employed. Financial restrictions included limiting private sector earnings, providing incentives to limit private sector activities, salary increases for public sector workers and performance-based payments. All financial restrictions intrinsically require well-established and adequate health financing systems to fund and monitor public and private sector activity. A combination of tax-based public financing, mandatory health insurance and private insurance might be necessary to counter the financial resource demands of this approach, while supervision, monitoring systems and transparent bureaucracies would be necessary to ensure that private sector activities and earnings are indeed limited and payments are matched by performance.
Allowing DP without restrictions was noted in countries like Indonesia and Egypt, where DP is routine and accepted. An interesting point to note is that in both countries, the productivity of physicians far exceeded the capacity of the public sector to employ them. Because of the low salaries offered in the public sector, physicians are allowed to supplement their incomes with private sector earnings. This approach is unlikely to be feasible in countries with health worker shortages. Considering the three options of total ban, allowing dual practice with restrictions and allowing it without restrictions, the most feasible for the LMICs is allowing it with restrictions. With health workers who are underpaid, in short supply and working in areas with a high burden of disease, they will scarcely be able to satisfy the demands of the public or the private sector alone.
WHO has released a report on DRGs that is useful as introduction to the concept and the design of payment systems.
The document consists of four parts:
Part 1 outlines definitions, terminology and the main conceptual aspects related to CBG and DRG.
Part 2 covers the assessment phase and highlights questions and issues that policy-makers should consider before taking the decision to introduce a CBG system.
Part 3 delves into the preparation phase by exploring policy and design aspects once a country has decided to introduce a CBG system.
Part 4 is concerned with the implementation phase and discusses implementation questions, requirements for system adjustments and the need for monitoring and revision in order to identify and address unintended impacts of a CBG system.

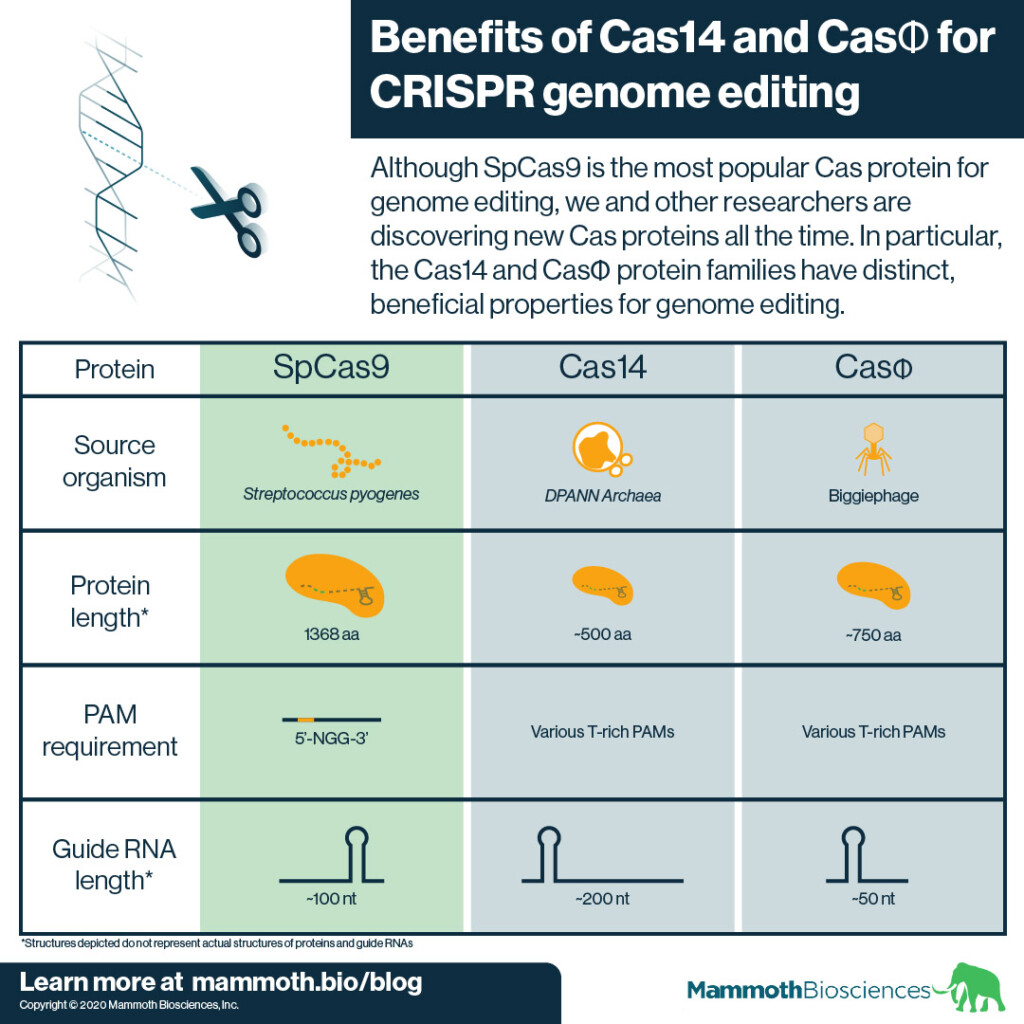
Improving CRISPR from Mammoth Biosciences;
Genome editing is the process researchers use to make targeted changes to an organism’s DNA (its genome). Scientists have used a variety of technologies for genome editing (see the history of genome editing here). However, since ~2012, CRISPR has made the genome editing processes much easier. CRISPR associated or “Cas” proteins drive this process. They are relatively easy to target to specific DNA sequences. They also work in many organisms.
Yet, the main Cas protein currently used for CRISPR genome editing, SpCas9, has limitations. In this post, we cover SpCas9’s limitations and how newly discovered Cas protein families, Cas14 and CasΦ, potentially overcome these limitations. We hope Cas14 and CasΦ will enable more efficient genome editing in diverse organisms and tissues.
From PNAS:
Changes in the way health insurers pay healthcare providers may not only directly affect the insurer’s patients but may also affect patients covered by other insurers.
This is the research question. And this is the result:
We use a payment reform in TM, which was randomly applied to some markets but not others, to study spillovers of healthcare payment reform. We find spillovers of the same sign and similar magnitude on privately insured MA patients. Naturally, our findings are specific to our setting; the existence, sign and magnitude of any spillovers may well vary across contexts.
Sounds good. However, there is a previous research question, which is the insurer's market share that allows to have the option to change the payment system. This former question is as relevant as the later one.

Hockney
Social isolation and loneliness are both terms that denote a degree of social disconnection. Social isolation is an objective state marked by few or infrequent social contacts. Loneliness is the subjective and distressing feeling of social isolation, often defined as the discrepancy between actual and desired level of social connection.
Social connection and connectedness encompass a variety of terms used in the scientific literature (for example, social support, social integration, social cohesion) that document the ways that being physically or emotionally connected to others can influence health and well-being.
In this HA Brief, the author explains that loneliness impact on health may be greater than we think. Rather than being alarming, she shows a description of the situation, the evidence and a proposal for policy agenda.
And if you are not convinced, than I would suggest this book:
The GTEx v8 data release represents a deep survey of both intra- and interindividual transcriptome variation across a large number of tissues. With 838 donors and 15,201 samples—approximately twice the size of the v6 release used in the previous set of GTEx Consortium papers—we have created a comprehensive resource of genetic variants that influence gene expression and splicing in cis. This substantially expands and updates the GTEx catalog of sQTLs, doubles the number of eGenes per tissue, and saturates the discovery of eQTLs with greater than twofold effect sizes in ~40 tissues. The fine-mapping data of GTEx cis-eQTLs provide a set of thousands of likely causal functional variants. While trans-QTL discovery and the characterization of sex- and population-specific genetic effects are still limited by sample size, analyses of the v8 data provide important insights into each.

Eliciting preferences for truth-telling in a survey of politicians
From PNAS:
Voters who would like to accurately evaluate the performance of politicians in office often rely on incomplete information and are uncertain whether politicians’ words can be trusted. Honesty is highly valued in politics because politicians who are averse to lying should in principle provide more trustworthy information. Despite the importance of honesty in politics, there is no scientific evidence on politicians’ lying aversion. We measured preferences for truth-telling in a sample of 816 elected politicians and study observable characteristics associated with honesty. We find that in our sample, politicians who are averse to lying have lower reelection rates, suggesting that honesty may not pay off in politics.
Therefore, in this case, truth-telling is a dominant non-rational strategy in politics. We still do need more evidence. Maybe the next presidential election will provide us a confirmation of this article.

The Price of Panic. How the Tyranny of Experts Turned a Pandemic into a Catastrophe
So, what caused the viral panic? The panic and lurching government overreach were inspired not so much by deaths people knew about firsthand, and not so much by the virus’s murky origins in China. They were sparked by a few forecasts that had the smell of science. The World Health Organization (WHO) favored a single, untested, apocalyptic model from Imperial College London. The United States government took its cues from the Institute for Health Metrics & Evaluation (IHME) at the University of Washington. We now know these models were so wrong they were like shots in the dark. After a few months, even the press admitted as much. But by then vast damage had been done.
But what of those experts? They treated predictive models—which are at best complex conjectures about future events—as if they were data. And then, when the models flopped, they began to massage the data. To get past this catastrophe we will need to forgive, but we should never forget. We should do whatever we can to dismantle such experts’ unchecked power over public policy.
These experts, however, could never have done so much damage without a gullible, self-righteous, and weaponized media that spread their projections far and wide. The press carpet-bombed the world with stories about impending shortages of hospital beds, ventilators, and emergency room capacity. They served up apocalyptic clickbait by the hour and the ton.
History shows that you will rarely lose your job making predictions if you’re wrong in the right direction. On the other hand, you may well lose it if you’re right in the wrong direction. Neither rulers nor subjects welcome the bearer of bad, but true, news. (Especially if it’s bad news for power-grabbing elites.)
Being wrong in the right direction, though, often reaps reward. Early pandemic models indicated that only prompt and massive state action could save us. The models were wrong—way off—but they were wrong in the right direction. They gave politicians justification for taking over almost every aspect of citizens’ lives. They gave the press clickbait galore. We’re not assuming malice here. We assume that many of these folks were moved by concern and even love for others. The issue is one of incentives and human nature, not bad intentions.
Our imagined pandemic model has made a huge mistake. How to explain that whopping error? In a perfect world, the experts who created the model, publicized, and used it to create public policy would reassess the assumptions they fed into the model—A, B, and C—find the mistake, and try new ones, which may better match the “observables.”
But we don’t live in a perfect world with perfect experts. What if experts are loath to admit that they were wrong? (We know that’s a real stretch, but stick with us here.) What if they have been feted by the press and promoted to positions of authority and power? They have other options besides the humiliating one of going back to the drawing board. For starters, such experts can stop using the word “predictions” to describe the forecasts that the model has been spitting out. Now they’re just “scenarios” or “guidelines” or “projections.” But these are just word games. There’s little daylight between a forecast, a prediction, a guess, a scenario, and a projection. All those words describe what the model is doing when it says, If A, B, and C are true, then something like X will happen, give or take a margin of error. If nothing like X happens, then something’s wrong with at least one of the model’s conceptual inputs, that is, with one of the propositions that that model assumed to be true. At least one of A, B, or C must be wrong.
It's only one view. Uncertainty is everywhere, and you may find snake-oil sellers in every corner.
PS. Tomorrow online presentation.
PS. Great post on pandemic models.
