Population health means the health outcomes of a defined group of people, as well as the distribution of health outcomes within the group.
Therefore, measuring and understanding the reasons for differences in health is a key factor for tackling them. Kindig paper is the most relevant, and this one reflects the begining.
From the post by Kings Fund :
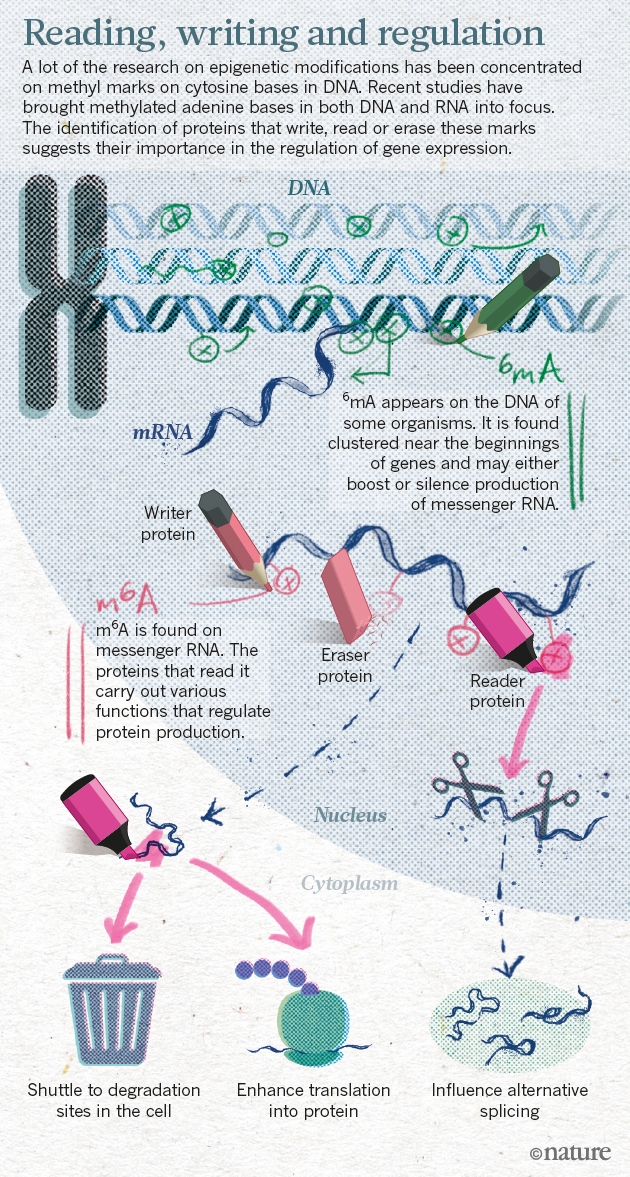
If epigenomics is crucial to discard the genetic predestination paradigm, now we can add a new 'omics to the paradigm: epitranscriptomics. Last February, Nature published interesting news related to recent scientific developments:
The epigenome helps to explain how cells with identical DNA can develop into the multitude of specialized types that make up different tissues. The marks help cells in the heart, for example, maintain their identity and not turn into neurons or fat cells. Misplaced epigenetic marks are often found in cancerous cells.
Chuan He and Tao Pan are two researchers that have been working on new ways of controlling gene expression
He and others have shown that a methyl group attached to adenine, one of the four bases in RNA, has crucial roles in cell differentiation, and may contribute to cancer, obesity and more. In 2015, He’s lab and two other teams uncovered the same chemical mark on adenine bases in DNA (methyl marks had previously been found only on cytosine), suggesting that the epigenome may be even richer than previously imagined.
The team had shown for the first time that RNA methylation was reversible, just like the marks found on DNA and histones.
Methylated adenine bases are the focus of research on gene expression.
Disciplines as diverse as economics, sociology, medicine, computer science, political science and physics have recently become interested in the interdependence of behaviours across the human social network. In particular, scientists have begun to ask whether our health and other behaviours are contagious, in that our decisions and actions affect the decisions and actions of our peers. If behavioural contagions exist, understanding how, when and to what extent they manifest in different behaviours will enable us to transition from independent intervention strategies to more effective interdependent interventions that incorporate individuals’ social contexts into their treatments
A new study offers some of the first hard evidence that health-related habits can spread — and so perhaps could be deliberately seeded and encouraged — by social influence and peer pressure. Previous research has sought such a contagious effect in factors such as obesity and smoking, but the results have been inconclusive.
Studies in social differences in health have a a new hurdle to tackle. How to boost social permeability? As Mackenback said in The Lancet on health inequalities: now it's personal.
PS. These are the results of the study in one figure:
Francis Fukuyama predicted 25 years ago the end of history, the triumph of liberal democracy and the arrival of post-ideological world, Now Y. N. Harari predicts the end of liberalism and the arrival of a post-humanism (?). All these efforts are useless in my opinion and the reason is obvious, those that predict the future don't have more information than any other human being. They could devote their time to fruitful initiatives.
If I knew that the second half of Homo Deus was devoted to the end of liberalism and the birth of a post-humanism, I wouldn't have read it. I always try to avoid snake-oil sellers. Reading is an asymmetric information game, the writer knows more than the reader. I would suggest to start a global snake-oil writers lists to reduce asymmetric information. The New Yorker publishes a sound review of the book,
Harari’s larger contention is that our homocentric creed, devoted to human liberty and happiness, will be destroyed by the approaching post-humanist horizon. Free will and individualism are, he says, illusions. We must reconceive ourselves as mere meat machines running algorithms, soon to be overtaken by metal machines running better ones. By then, we will no longer be able to sustain our comforting creed of “autonomy,” the belief, which he finds in Rousseau, that “I will find deep within myself a clear and single inner voice, which is my authentic self,” and that “my authentic self is completely free.” In reality, Harari maintains, we have merely a self-deluding, “narrating self,” one that recites obviously tendentious stories, shaped by our evolutionary history to help us cope with life. We are—this is his most emphatic point—already machines of a kind, robots unaware of our own programming. Humanism will be replaced by Dataism; and if the humanist revolution made us masters the Dataist revolution will make us pets.
Does this makes any sense? Is it possible to remain as the current best seller with such a message?
Parkinson’s disease, a nervous system disorder impacting movement
Late-onset Alzheimer’s disease, a progressive brain disorder that destroys memory and thinking skills
Celiac disease, a disorder resulting in the inability to digest gluten
Alpha-1 antitrypsin deficiency, a disorder that raises the risk of lung and liver disease
Early-onset primary dystonia, a movement disorder involving involuntary muscle contractions and other uncontrolled movements
Factor XI deficiency, a blood clotting disorder
Gaucher disease type 1, an organ and tissue disorder
Glucose-6-Phosphate Dehydrogenase deficiency, also known as G6PD, a red blood cell condition
Hereditary hemochromatosis, an iron overload disorder
Hereditary thrombophilia, a blood clot disorder
Meanwhile NASEM recommends a decision framework for the use of genetic tests in clinical care:
1. Define genetic test scenarios on the basis of the clinical setting, the purpose of the test, the population, the outcomes of interest, and comparablealternative methods.
2. For each genetic test scenario, conduct an initial structured assessment to determine whether the test should be covered, denied, or subject to additional evaluation.
3. Conduct or support evidence-based systematic reviews for genetic test scenarios that require additional evaluation.
4. Conduct or support a structured decision process to produce clinical guidance for a genetic test scenario.
5. Publicly share resulting decisions and justification about evaluated genetic test scenarios, and retain decisions in a repository.
6. Implement timely review and revision of decisions on the basis of new data.
7. Identify evidence gaps to be addressed by research.
If you want further details, check Mathew Herper blog. My first impression after reading it is that this move, paves the way for recreational genetic testing. An approach that should be completely banned by legislation. If FDA has done so, let's wait for what it may happen in Europe where the regulator is still planning a change of the regulation in 2022!!! Meanwhile, the door is open (to the worst for citizens).
There are big questions unanswered in health policy, and the social willingness to pay for a costly and effective technology is one of them. In a recent article, a description and controversies of NHS budget impact policies are explained:
The budget impact test means that technologies costing the NHS more than an additional £20m a year will be “slow tracked,” regardless of their cost effectiveness or other social or ethical values. This risks undermining the existing opportunity costs framework.
Therefore if there is a costly and effective therapy that has an impact budget greater than 20m, than next steps are uncertain in UK. This is the setting.
Really this affects all health politicians, and the issue is related to prioritisation and price regulation. The "solution" to the first issue is to delay prioritisation to the next minister, and what it is possible is to renegotiate prices of drugs. As I have said many times, prices are a fiction, because what it is under negotiation is a contract with the government, therfore the whole amount (p·q).
Budget impact is essentially the price per patient multiplied by the number of patients treated. Yet the prevalence of someone’s condition should not determine their access to treatment. The principle of equity means that like cases should be treated as like; the NHS Constitution requires the NHS to respond to the clinical needs of patients as individuals.
Righ now in Catalonia cost-effectiveness is a also a fiction, since prices are confidential, and it is not possible to estimate the ratio. Budget impact is the option.
Approximately 12-14 investigational gene therapies for
additional ultra-rare conditions and some for more common conditions, such as
haemophilia and sickle cell disease, are progressing through the developmental pathway
and are expected to reach regulatory approval within the next 2-3 years
These therapies rely mostly on viral vector techniques, therefore they don't take into account the coming genome editing, the most disruptive one and the most recent as well. If this new technologies reach the market, how should be paid and applied?. This is what a recent report explains and gives details for decision makers. It is really welcome, the issue deserves a deeper understanding.
Situation in Europe
Glybera and Strimvelis, have been granted marketing authorization in the European Union by the European Medicines Agency (EMA):
- Glybera was approved by the EMA in 2012, but has since become the world’s most expensive short-term treatment (Adams, 2016), and as such has not been widely successful - it has only been used by one patient, with the prescribing clinician overcoming steep bureaucratic hurdles to obtain insurer funding (Abou-El-Enein et al., 2016a).
- Strimvelis received marketing authorization in 2016. Patients can currently only be treated in Milan, due to the treatment’s extremely short shelf life which dictates that cells must be infused back into the patient in less than six hours.
More efforts should be devoted to understand this emerging market and assess its value.
The inequality frame is usually flawed, and this is specially clear when the metholodogy and data to support the statements are biased. Let me suggest today this article that summarises perfectly common misunderstandings on this relationship. It would be a great input for a review and remake of recent papers.
The summary:
What is already known about this topic? A large body of research has examined the
association between income inequality and average health. A separate body of research has
explored income disparities in health. These two traditions should be seen as complementary,
because high and rising income inequality is unlikely to affect the health of all socioeconomic
groups equally.
What is added by this report? Although plausible theories suggest that rising income
inequality can affect both average health and health disparities, empirical tests provide only
modest support for some of these theories. We argue that understanding the effects of income
inequality on health requires attention to mechanisms that affect the health of different income
groups, thus changing average health, disparities in health, or both.
What are the implications for public health practice, policy, and research? Progress is
likely to require disentangling direct effects of rising income inequality, which operate through
changes in an individual’s own income, from indirect effects, which operate through changes
in other people’s income. Indirect effects of rising income inequality may change a society’s
political and economic institutions, social cohesion, culture, and norms of behavior, all of
which can then affect individuals’ health even if their income remains unchanged.
PS. If someone needs an estimate of morbidity, please avoid inconsistent approaches. If someone needs policy guidance don't trust on cross-sectional data on such a difficult issue.
The Nuffield Council has released a key document on ethical implications of genome editing. You'll notice that it is an open document, a work in progress because technology is evolving. If you want an excerpt check this short guide.
It should be remembered that most prospective technologies fail, and that some lead to undesirable consequences, a fact often obscured by ‘whig’ histories that reconstruct the history of successful technologies and their beneficial social consequences. Scientific discovery and technological innovation is important but not inevitable. Most important among the factors shaping technological development is human agency. It is human agency, in terms of decisions that are made about directions of research, funding and investment, the setting of legal limits and regulatory principles, the design of institutions and programmes, and the desire for or acceptance of different possible states of affairs, that will determine whether, and which, prospective technologies emerge and, ultimately,
their historical significance.
Nuffield council work is of interest, meanwhile, China is already testing CRISPR technology in humans, no ethical concerns...
Last summer the Office of Health Economics released an inspiring paper on the value of diagnostic information related to companion diagnostics and next generation sequencing genomic tests. I read it recently and its appproach sheds additional light on a difficult issue:
Traditional cost-effectiveness analysis conducted as part of HTA focuses on three key elements:
1. Life years gained
2. Improvements in patient quality of life
3. Cost-savings within the healthcare system (also called “cost-offsets”).
Elements 1 and 2 are often combined in the quality-adjusted life year (QALY) by HTA bodies.
Elements 1, 2, and 3, plus the cost of the technology, are then used to assess the cost effectiveness of the technology.
The next element most often included is “productivity” or “time value”, reflecting gains and losses related to the value of the patient’s time either when receiving medical care or related to the impact of absenteeism or presenteeism due to illness. Another element - less commonly measured - is nonmedical cost-savings outside the healthcare sector, such as transport costs and family caregiving.
Based on our systematic literature review, we identified and defined five additional elements
related to the value of knowing and the value of information:
• Reduction in uncertainty - additional value from knowing a technology is more likely to work
• Value of hope - willingness to accept greater risk given a chance for a cure
• Real option value - the value of benefiting from future technologies due to life extension
• Insurance value - psychic value provided by invention of an innovative medical product and by the accompanying financial risk protection afforded by a new treatment
• Scientific spillovers - value due to other innovations that become possible once a new technology has been proven to work.
I have discussed many times such additional issues, specially the real option value. Unfortunately measurement of such items are not that easy. Anyway, it's good to take into account and let's hope new developments on this topic.
Today I would like to suggest you to read Barack Obama in his farewell speech. It's an inspiring piece to understand US and democracies in general. Inequality, racism and polarization are the three key isues to tackle.
He said:
For too many of us, it’s become safer to retreat into our own bubbles, whether in our neighborhoods or college campuses or places of worship or our social media feeds, surrounded by people who look like us and share the same political outlook and never challenge our assumptions. The rise of naked partisanship, increasing economic and regional stratification, the splintering of our media into a channel for every taste – all this makes this great sorting seem natural, even inevitable. And increasingly, we become so secure in our bubbles that we accept only information, whether true or not, that fits our opinions, instead of basing our opinions on the evidence that’s out there.
This trend represents a third threat to our democracy. Politics is a battle of ideas; in the course of a healthy debate, we’ll prioritize different goals, and the different means of reaching them. But without some common baseline of facts; without a willingness to admit new information, and concede that your opponent is making a fair point, and that science and reason matter, we’ll keep talking past each other, making common ground and compromise impossible.
Without a common baseline of facts there is no possibility to talk to your political opponent. Nowadays, fake news like health privatization are continuously spreading without any foundation. Our health minister speaks incredibly about that in our Parliament. Such obsession has driven to submit a new unnecessary law on health contracting.We are now in an obsession focused policy era.
To understand this phenomena, Sunstein wrote a book in 2008, before thee term post-truth era, that explains the basics and what to do. Cass Sunstein says in the book:
Rumors are nearly as old as human history, but with the rise of the Internet, they have become ubiquitous. In fact we are now awash in them. False rumors are especially troublesome; they impose real damage on individuals and institutions, and they often resist correction. They can threaten careers, relationships, policies, public officials, democracy, and sometimes even peace itself. Many of the most pervasive rumors involve governments—what officials are planning and why.
This small book has two goals. The first is to answer these questions: Why do ordinary human beings accept rumors, even false, destructive, and bizarre ones? Why do some groups, and even nations, accept rumors that other groups and nations deem preposterous? The second is to answer this question: What can we do to protect ourselves against the harmful effects of false rumors? As we shall see, part of the answer lies in recognizing that a “chilling effect” on those who would spread destructive falsehoods can be a truly excellent idea, especially if those falsehoods amount to libel.
Sensible people believe rumors, whether or not they are true. On the Internet, self-interested, malicious, and altruistic propagators find it increasingly easy to spread rumors about prominent people and institutions. Such rumors cast doubt on their target’s honesty, decency, fairness, patriotism, and sometimes even sanity; often they portray public figures as fundamentally confused or corrupt. Those who are not in the public sphere are similarly vulnerable.
Rumor transmission frequently occurs as a result of cascade effects and group polarization. Indeed, rumors spread as a textbook example of an informational cascade: imperfectly or entirely uninformed people accept a rumor that they hear from others, and as more and more people accept that rumor, the informational signal becomes very strong, and it is hard for the rest of us to resist it, even if it is false.
Group polarization also plays a large role, as people strengthen their commitment to a rumor simply because of discussions with like-minded others.
If you want people to move away from their prior convictions, and to correct a false rumor, it is best to present them not with the opinions of their usual adversaries, whom they can dismiss, but instead with the views of people with whom they closely identify
The signal of the rumor may be so strong that though reality is absolutely different, and everybody is finally conceding it the value of truth. This is sadly what has happened to health privatization debate.
Too often people talk about the value of health, and few are those that try to measure it. Now you have the opportunity to have a look at the book that summarises the state of the art on measuring health from different perspectives, clinical and research, epidemiology and economics (resource allocation). The implications of health in well being are explored, and the author says:
Valuing health states by their average consequences for well-being has the unfortunate implication that disabilities count as significant health problems only if the people who have them are significantly worse off than the people without them. With respect to disabilities, such as blindness, to which people adapt, this implication leaves the health analyst with a choice between asserting falsely that the blind necessarily have lower levels of well-being or asserting falsely that blindness is not a serious disability.
This unfortunate implication, coupled with the difficulties in measuring the value of health by eliciting preferences or by measuring subjective experience, raises doubts about the project of valuing health by its bearing on well-being, which chapter
10 explores. The value of health differs in important ways from well-being and indeed appears to be easier to measure than well-being.
And we all agree that health is a crucial factor for well-being, though its measurement is uncertain up to now.
Last book by Gary Taubes takes a difficult way, how to demonstrate sugar as a toxic substance for our health. Although he tries to show evidence for his words, he finally concedes the following conclusion:
Ultimately and obviously, the question of how much is too much becomes a personal decision, just as we all decide as adults what level of alcohol, caffeine, or cigarettes we’ll ingest. I’ve argued here that enough evidence exists for us to consider sugar very likely to be a toxic substance, and to make an informed decision about how best to balance the likely risks with the benefits. To know what those benefits are, though, it helps to see how life feels without sugar.
The "very likely" expression is crucial. Unfortunately we don't have a explicit causal explanation of the impact of sugar on metabolic syndrome, for example. I think that epigenetics will provide neew perspectives on the issue, however we will have to wait. Meanwhile reducing exposure is the best advice.
K. J. Arrow passed away this Wednesday. He is one of the giants of economics and the founder of health economics. It is difficult to summarise his works in few words. You'll find obituaries in the Post and NYT. Josep M. Colomer has written an interesting post in his blog (social choice perspective). Tony Culyer has published also his obituary (health economics perspective)
An interview in a recent book reviews his works and opinions. Regarding healt economics, he says:
I was asked to study, as a theoretical economist, health care. This was a paper that I regard very highly, one of the best things I ever did. I think I mentioned that in fact, afair amount of my research is the result of people asking me these kinds of questions. I studied Social Choice because somebody asked me a question. A now retired professor, Victor Fuchs, was then at the Ford Foundation, and they wanted to get studies done of social problems. They wanted studies of welfare—in the ordinary sense of the word—of medical care and of education. For each of these areas, they wanted one study by somebody who had worked in the field and one by a theorist, and I’m a theorist who had not necessarily worked with people.
In my case, I was asked to work on medical care. I read up on the literature, and gradually a pattern emerged that essentially the parties know different things. The physician knows a lot that the patient doesn’t, and therefore the patient can’t check on the quality of medical care in the same way we buy a loaf of bread. It’s not like I’ll buy that loaf again. But with medical care, you can’t be sure because you don’t know that much. It’s the same thing between the insurer and the physician or the patient. So I said that with medical care, noneconomic factors, essentially ethical codes, play a role in keeping the system together. But I didn’t have a theory at the time, I just had a statement. It was pretty clear to me that non-economic factors do play a major role. What is considered good practice, that’s what keeps the system going. The trouble is that I’ve seen the limits of economic analysis. I could see one solution, but it was very different from market kinds of solutions. But I did have a theory about it.
When I look at other people, they don’t have theories either, or they have rather vague theories. When I try to impart this to students, of course it’s a very confusing message. That’s one of the reasons I don’t think I’ve been a great teacher. I’ve perhaps had students who did appreciate what I was doing, although they tended to pick up the more technical parts of it. I’m a little disappointed they haven’t tried to tackle the broader picture. If they’re working with it, they’ve done very fine work, going well beyond what I did. So I’d say that would be a rather lengthy answer to your question. I see myself primarily as a scholar, as a thinker about things, trying to enlist others in this thinking. Yes, I think I would say that more so than others.